

Receiving hospital characteristics associated with survival after out-of-hospital cardiac arrest
- PMID: 20071070
- PMCID: PMC2856722
- DOI: 10.1016/j.resuscitation.2009.12.006
Receiving hospital characteristics associated with survival after out-of-hospital cardiac arrest
Abstract
Aim: Survival after out-of-hospital cardiac arrest (OOHCA) varies between regions, but the contribution of different factors to this variability is unknown. This study examined whether survival to hospital discharge was related to receiving hospital characteristics, including bed number, capability of performing cardiac catheterization and hospital volume of OOHCA cases.
Material and methods: Prospective observational database of non-traumatic OOHCA assessed by emergency medical services was created in 8 US and 2 Canadian sites from December 1, 2005 to July 1, 2007. Subjects received hospital care after OOHCA, defined as either (1) arriving at hospital with pulses, or (2) arriving at hospital without pulses, but discharged or died > or =1 day later.
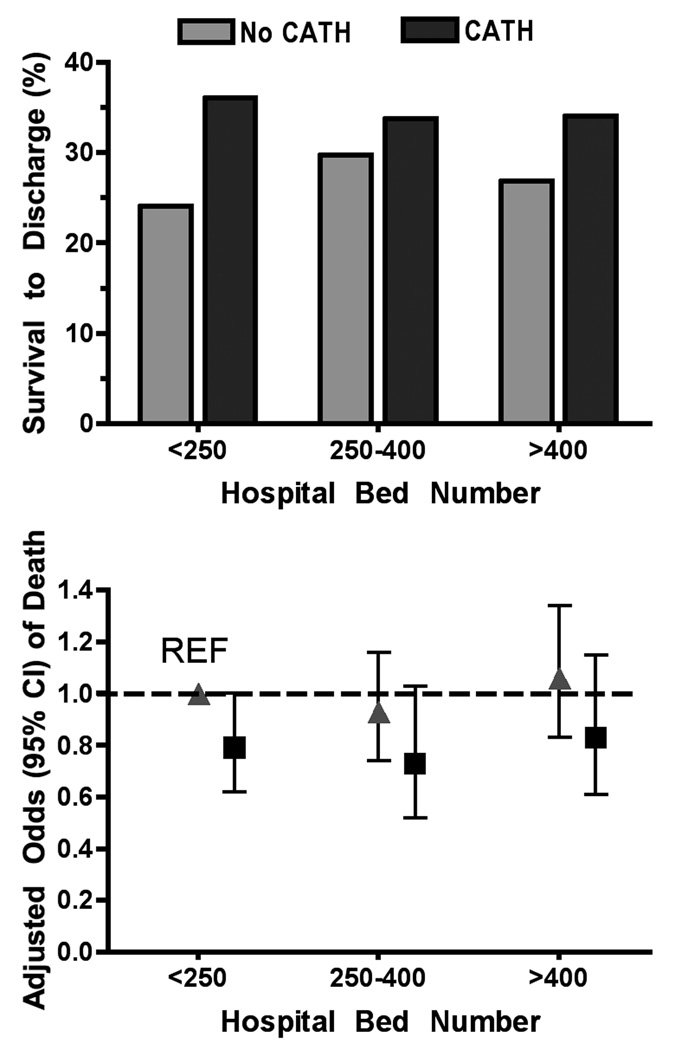
Results: A total of 4087 OOHCA subjects were treated at 254 hospitals, and 32% survived to hospital discharge. A majority of subjects (68%) were treated at 116 (46%) hospitals capable of cardiac catheterization. Unadjusted survival to discharge was greater in hospitals performing cardiac catheterization (34% vs. 27%, p=0.001), and in hospitals that received > or =40 patients/year compared to those that received <40 (37% vs. 30%, p=0.01). Survival was not associated with hospital bed number, teaching status or trauma center designation. Length of stay (LOS) for surviving subjects was shorter at hospitals performing cardiac catheterization (p<0.01). After adjusting for all variables, there were no independent associations between survival or LOS and hospital characteristics.
Conclusions: Some subsets of hospitals displayed higher survival and shorter LOS for OOHCA subjects but there was no independent association between hospital characteristics and outcome.
Copyright 2010 Elsevier Ireland Ltd. All rights reserved.
Figures
Comment in
-
Statistical considerations in assessing the impact of hospital characteristics and cardiac arrest survival.Resuscitation. 2010 Nov;81(11):1586; author reply 1586-7. doi: 10.1016/j.resuscitation.2010.03.044. Epub 2010 Jul 23. Resuscitation. 2010. PMID: 20655138 No abstract available.
References
-
- Hypothermia after Cardiac Arrest Study Group. Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. N Engl J Med. 2002;346:549–556. - PubMed
-
- Bernard SA, Gray TW, Buist MD, Jones BM, Silvester W, Gutteridge G, Smith K. Treatment of comatose survivors of out-of-hospital cardiac arrest with induced hypothermia. N Engl J Med. 2002;346:557–563. - PubMed
-
- Sunde K, Pytte M, Jacobsen D, Mangschau A, Jensen LP, Smedsrud C, Draegni T, Steen PA. Implementation of a standardised treatment protocol for post resuscitation care after out-of-hospital cardiac arrest. Resuscitation. 2007;73:29–39. - PubMed
Publication types
MeSH terms
Grants and funding
- U01 HL077866/HL/NHLBI NIH HHS/United States
- U01 HL077871/HL/NHLBI NIH HHS/United States
- HL077867/HL/NHLBI NIH HHS/United States
- 5U01 HL077/HL/NHLBI NIH HHS/United States
- HL077887/HL/NHLBI NIH HHS/United States
- U01 HL077881/HL/NHLBI NIH HHS/United States
- HL077873/HL/NHLBI NIH HHS/United States
- HL077871/HL/NHLBI NIH HHS/United States
- HL077881/HL/NHLBI NIH HHS/United States
- HL077908/HL/NHLBI NIH HHS/United States
- U01 HL077887/HL/NHLBI NIH HHS/United States
- U01 HL077885/HL/NHLBI NIH HHS/United States
- CAPMC/ CIHR/Canada
- U01 HL077865/HL/NHLBI NIH HHS/United States
- U01 HL077863/HL/NHLBI NIH HHS/United States
- U01 HL077908/HL/NHLBI NIH HHS/United States
- HL077872/HL/NHLBI NIH HHS/United States
- HL077866/HL/NHLBI NIH HHS/United States
- U01 HL077873/HL/NHLBI NIH HHS/United States
- U01 HL077867/HL/NHLBI NIH HHS/United States
- HL077885/HL/NHLBI NIH HHS/United States
- HL077865/HL/NHLBI NIH HHS/United States
- U01 HL077872/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
