

Perioperative use of cuffed endotracheal tubes is advantageous in young pediatric burn patients
- PMID: 20071090
- PMCID: PMC3045666
- DOI: 10.1016/j.burns.2009.11.011
Perioperative use of cuffed endotracheal tubes is advantageous in young pediatric burn patients
Abstract
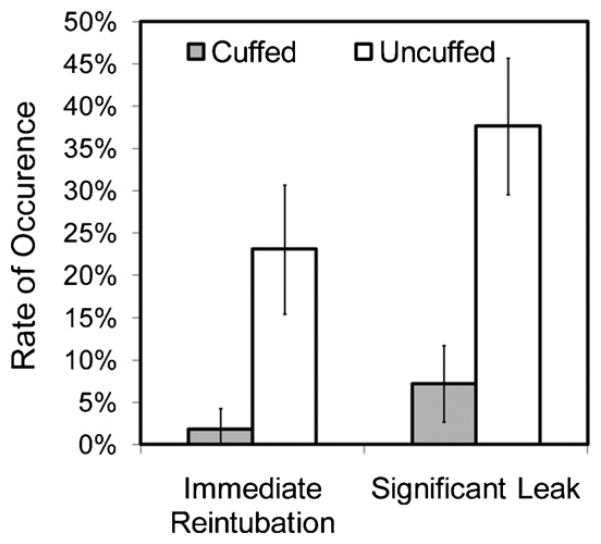
Uncuffed endotracheal tubes traditionally have been preferred over cuffed endotracheal tubes in young pediatric patients. However, recent evidence in elective pediatric surgical populations suggests otherwise. Because young pediatric burn patients can pose unique airway and ventilation challenges, we reviewed adverse events associated with the perioperative use of cuffed and uncuffed endotracheal tubes. We retrospectively reviewed 327 cases of operating room endotracheal intubation for general anesthesia in burned children 0-10 years of age over a 10-year period. Clinical airway outcomes were compared using multivariable logistic regression, controlling for relevant patient and injury characteristics. Compared to those receiving cuffed tubes, children receiving uncuffed tubes were significantly more likely to demonstrate clinically significant loss of tidal volume (odds ratio 10.62, 95% confidence interval 2.2-50.5) and require immediate reintubation to change tube size/type (odds ratio 5.54, 95% confidence interval 2.1-13.6). No significant differences were noted for rates of post-extubation stridor. Our data suggest that operating room use of uncuffed endotracheal tubes in such patients is associated with increased rates of tidal volume loss and reintubation. Due to the frequent challenge of airway management in this population, strategies should emphasize cuffed endotracheal tube use that is associated with lower rates of airway manipulation.
2009 Elsevier Ltd and ISBI. All rights reserved.
Figures
References
-
- Fisher DM. Anesthesia equipment for pediatrics. In: Gregory GA, editor. Pediatr Anesth. 4th ed. Churchill Livingstone; New York: 2001. pp. 207–8.
-
- Motoyama EK. Endotracheal intubation. In: Motoyama EK, Davis PJ, editors. Smith's anesthesia for infants and children. 5th ed. C.V. Mosby; St. Louis, MO: 1990. pp. 269–75.
-
- Calhoun K. Long-term airway sequelae in a pediatric burn population. Laryngoscope. 1988;98:721–5. - PubMed
-
- Khine H. Comparison of cuffed and uncuffed endotracheal tubes in young children during general anesthesia. Anesthesiology. 1997;86(3):627–31. - PubMed
-
- Newth CJL, Rachman B, Patel N, Hammer J. The use of cuffed versus uncuffed endotracheal tubes in pediatric intensive care. J Pediatr. 2004;144:333–7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
