

Chronic Mycobacterium abscessus infection and lung function decline in cystic fibrosis
- PMID: 20071249
- PMCID: PMC3837580
- DOI: 10.1016/j.jcf.2009.12.001
Chronic Mycobacterium abscessus infection and lung function decline in cystic fibrosis
Abstract
Background: Although nontuberculous mycobacteria (NTM) are recognized pathogens in cystic fibrosis (CF), associations with clinical outcomes remain unclear.
Methods: Microbiological data was obtained from 1216 CF patients over 8years (481+/-55patients/year). Relationships to clinical outcomes were examined in the subset (n=271, 203+/-23 patients/year) with longitudinal data.
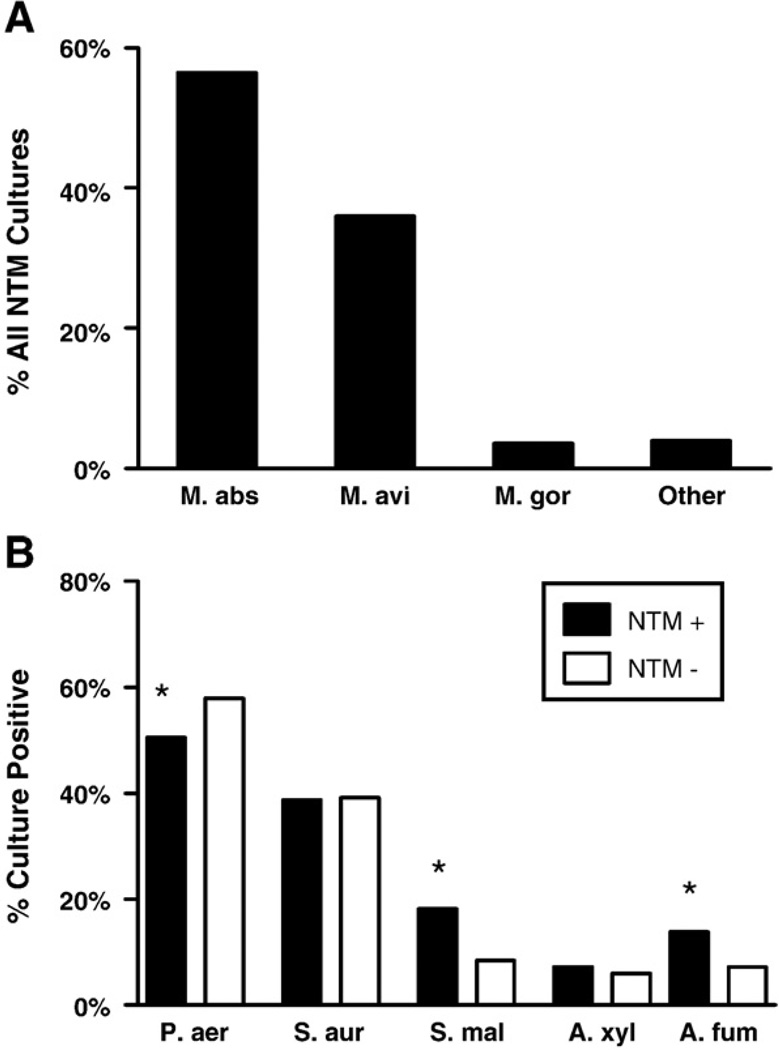
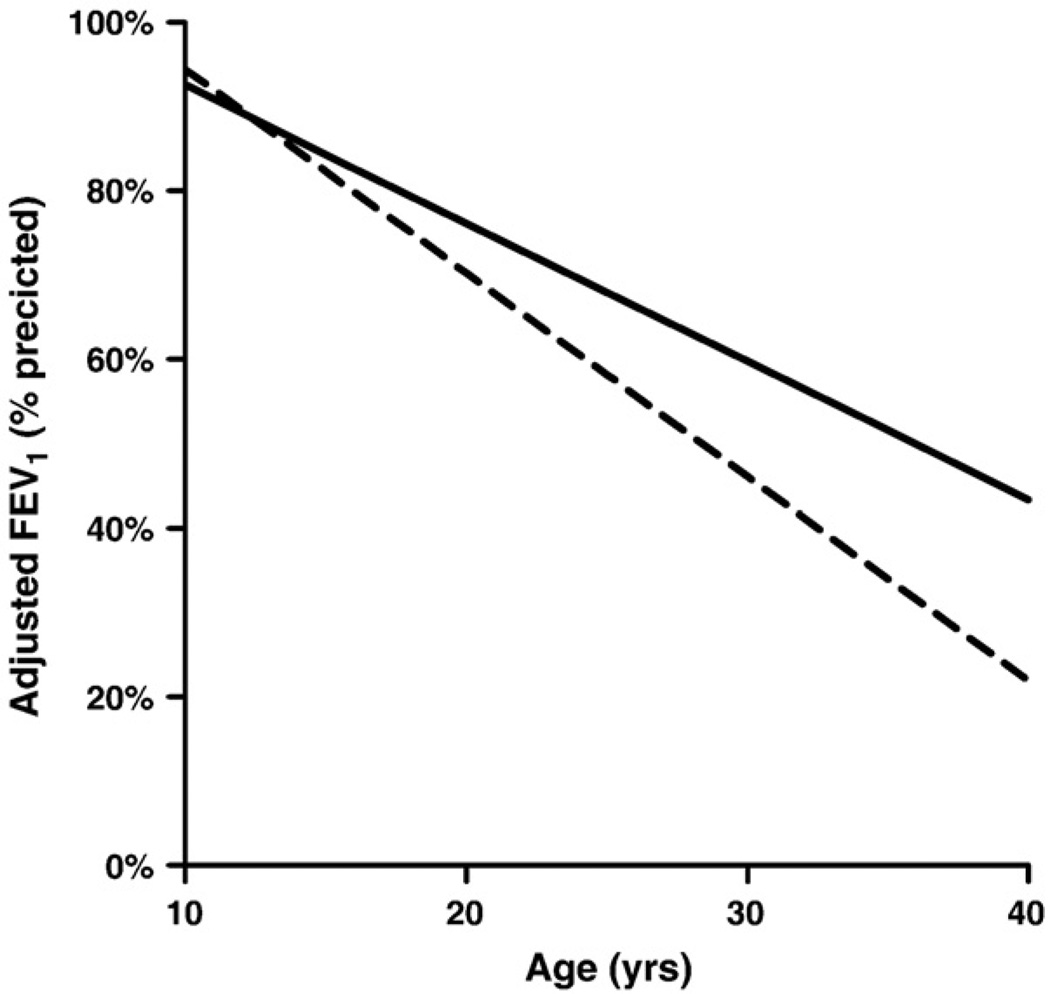
Results: Five hundred thirty-six of 4862 (11%) acid-fast bacilli (AFB) cultures grew NTM, with Mycobacterium abscessus (n=298, 55.6%) and Mycobacterium avium complex (n=190, 35.4%) most common. Associated bacterial cultures grew Stenotrophomonas or Aspergillus species more often when NTM were isolated (18.2% vs. 8.4% and 13.9% vs. 7.2%, respectively, p<0.01). After controlling for confounders, patients with chronic M. abscessus infection had greater rates of lung function decline than those with no NTM infection (-2.52 vs. -1.64% predicted FEV(1)/year, p<0.05).
Conclusions: NTM infection is common in CF and associated with particular pathogens. Chronic M. abscessus infection is associated with increased lung function decline.
Copyright (c) 2009 European Cystic Fibrosis Society. Published by Elsevier B.V. All rights reserved.
Figures
References
-
- Glassroth J. Pulmonary disease due to nontuberculous mycobacteria. Chest. 2008 Jan;133(1):243–251. - PubMed
-
- Razvi S, Saiman L. Nontuberculous mycobacteria in cystic fibrosis. Pediatr Infect Dis J. 2007 Mar;26(3):263–264. - PubMed
-
- Olivier KN. The natural history of nontuberculous mycobacteria in patients with cystic fibrosis. Paediatr Respir Rev. 2004;(5 Suppl A):S213–S216. - PubMed
-
- Olivier KN, Weber DJ, Wallace RJ, Jr, Faiz AR, Lee JH, Zhang Y, et al. Nontuberculous mycobacteria. I: multicenter prevalence study in cystic fibrosis. Am J Respir Crit Care Med. 2003 Mar 15;167(6):828–834. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
