

A novel method to adjust efficacy estimates for uptake of other active treatments in long-term clinical trials
- PMID: 20072614
- PMCID: PMC2798963
- DOI: 10.1371/journal.pone.0008580
A novel method to adjust efficacy estimates for uptake of other active treatments in long-term clinical trials
Erratum in
- PLoS One. 2010;5(1). doi: 10.1371/annotation/54433693-04e0-4f30-9a99-38fe3c5bb16b
Abstract
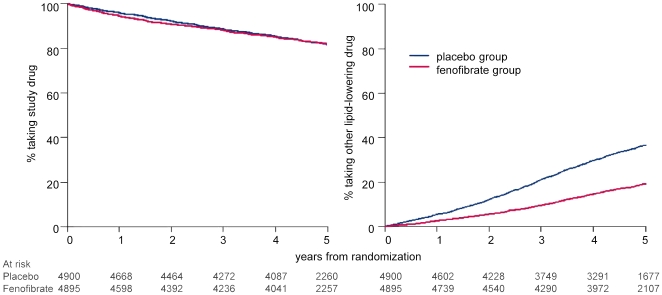
Background: When rates of uptake of other drugs differ between treatment arms in long-term trials, the true benefit or harm of the treatment may be underestimated. Methods to allow for such contamination have often been limited by failing to preserve the randomization comparisons. In the Fenofibrate Intervention and Event Lowering in Diabetes (FIELD) study, patients were randomized to fenofibrate or placebo, but during the trial many started additional drugs, particularly statins, more so in the placebo group. The effects of fenofibrate estimated by intention-to-treat were likely to have been attenuated. We aimed to quantify this effect and to develop a method for use in other long-term trials.
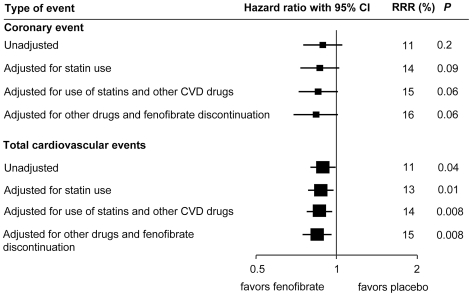
Methodology/principal findings: We applied efficacies of statins and other cardiovascular drugs from meta-analyses of randomized trials to adjust the effect of fenofibrate in a penalized Cox model. We assumed that future cardiovascular disease events were reduced by an average of 24% by statins, and 20% by a first other major cardiovascular drug. We applied these estimates to each patient who took these drugs for the period they were on them. We also adjusted the analysis by the rate of discontinuing fenofibrate. Among 4,900 placebo patients, average statin use was 16% over five years. Among 4,895 assigned fenofibrate, statin use was 8% and nonuse of fenofibrate was 10%. In placebo patients, use of cardiovascular drugs was 1% to 3% higher. Before adjustment, fenofibrate was associated with an 11% reduction in coronary events (coronary heart disease death or myocardial infarction) (P = 0.16) and an 11% reduction in cardiovascular disease events (P = 0.04). After adjustment, the effects of fenofibrate on coronary events and cardiovascular disease events were 16% (P = 0.06) and 15% (P = 0.008), respectively.
Conclusions/significance: This novel application of a penalized Cox model for adjustment of a trial estimate of treatment efficacy incorporates evidence-based estimates for other therapies, preserves comparisons between the randomized groups, and is applicable to other long-term trials. In the FIELD study example, the effects of fenofibrate on the risks of coronary heart disease and cardiovascular disease events were underestimated by up to one-third in the original analysis.
Trial registration: Controlled-Trials.com ISRCTN64783481.
Conflict of interest statement
Figures
Similar articles
-
Fenofibrate Intervention and Event Lowering in Diabetes (FIELD) study: baseline characteristics and short-term effects of fenofibrate [ISRCTN64783481].Cardiovasc Diabetol. 2005 Aug 22;4:13. doi: 10.1186/1475-2840-4-13. Cardiovasc Diabetol. 2005. PMID: 16111499 Free PMC article. Clinical Trial.
-
"If it ain't broke, don't fix it": a commentary on the positive-negative results of the ACCORD Lipid study.Cardiovasc Diabetol. 2010 Jun 15;9:24. doi: 10.1186/1475-2840-9-24. Cardiovasc Diabetol. 2010. PMID: 20550659 Free PMC article.
-
Fenofibrate: a review of its lipid-modifying effects in dyslipidemia and its vascular effects in type 2 diabetes mellitus.Am J Cardiovasc Drugs. 2011 Aug 1;11(4):227-47. doi: 10.2165/11207690-000000000-00000. Am J Cardiovasc Drugs. 2011. PMID: 21675801 Review.
-
Is fenofibrate a cost-saving treatment for middle-aged individuals with type II diabetes? An economic analysis of the FIELD Study.Int J Cardiol. 2008 Jun 23;127(1):51-6. doi: 10.1016/j.ijcard.2007.04.040. Epub 2007 Jun 21. Int J Cardiol. 2008. PMID: 17586072
-
Update on PPAR agonists: the clinical significance of FIELD and PROACTIVE.Curr Atheroscler Rep. 2007 Jan;9(1):64-71. doi: 10.1007/BF02693930. Curr Atheroscler Rep. 2007. PMID: 17169249 Review.
Cited by
-
Fenofibrate: a review of its use in dyslipidaemia.Drugs. 2011 Oct 1;71(14):1917-46. doi: 10.2165/11208090-000000000-00000. Drugs. 2011. PMID: 21942979 Review.
-
Cardiovascular risk scores do not account for the effect of treatment: a review.Heart. 2011 May;97(9):689-97. doi: 10.1136/hrt.2010.220442. Heart. 2011. PMID: 21474616 Free PMC article. Review.
-
Prediction of Cardiovascular Disease Risk Accounting for Future Initiation of Statin Treatment.Am J Epidemiol. 2021 Oct 1;190(10):2000-2014. doi: 10.1093/aje/kwab031. Am J Epidemiol. 2021. PMID: 33595074 Free PMC article.
-
Using marginal structural models to adjust for treatment drop-in when developing clinical prediction models.Stat Med. 2018 Dec 10;37(28):4142-4154. doi: 10.1002/sim.7913. Epub 2018 Aug 2. Stat Med. 2018. PMID: 30073700 Free PMC article.
-
Impact of metabolic syndrome and its components on cardiovascular disease event rates in 4900 patients with type 2 diabetes assigned to placebo in the FIELD randomised trial.Cardiovasc Diabetol. 2011 Nov 21;10:102. doi: 10.1186/1475-2840-10-102. Cardiovasc Diabetol. 2011. PMID: 22104275 Free PMC article. Clinical Trial.
References
-
- White IR. Uses and limitations of randomization-based efficacy estimators. Stat Methods Med Res. 2005;14:327. - PubMed
-
- Yamaguchi T, Ohashi Y. Adjusting for differential proportions of second-line treatment in cancer clinical trials. Part I: Structural nested models and marginal structural models to test and estimate treatment arm effects. Stat Med. 2004;23:1991–2003. - PubMed
-
- Heritier SR, Gebski VJ, Keech AC. Inclusion of patients in clinical trial analysis: the intention-to-treat principle. Med J Aust. 2003;179:438–440. - PubMed
-
- Sheiner LB, Rubin DB. Intention-to-treat analysis and the goal of clinical trials. Clin Pharmacol Ther. 1995;56:6–10. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
