

Gel versus capillary electrophoresis genotyping for categorizing treatment outcomes in two anti-malarial trials in Uganda
- PMID: 20074380
- PMCID: PMC2817701
- DOI: 10.1186/1475-2875-9-19
Gel versus capillary electrophoresis genotyping for categorizing treatment outcomes in two anti-malarial trials in Uganda
Abstract
Background: Molecular genotyping is performed in anti-malarial trials to determine whether recurrent parasitaemia after therapy represents a recrudescence (treatment failure) or new infection. The use of capillary instead of agarose gel electrophoresis for genotyping offers technical advantages, but it is unclear whether capillary electrophoresis will result in improved classification of anti-malarial treatment outcomes.
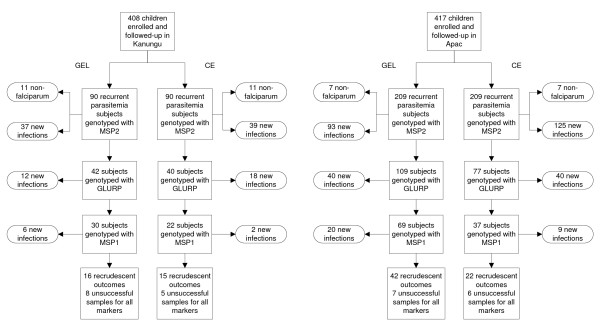
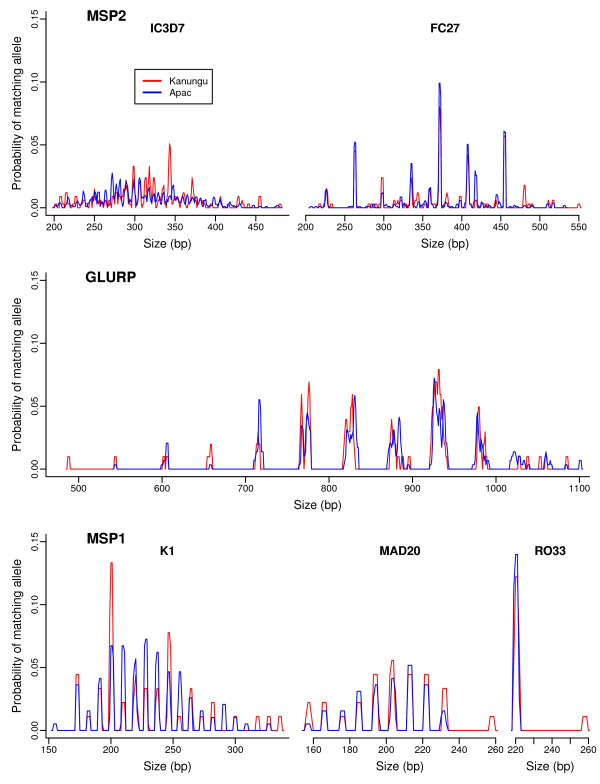
Methods: Samples were genotyped using both gel and capillary electrophoresis from randomized trials of artemether-lumefantrine (AL) vs. dihydroartemisinin-piperaquine (DP) performed in two areas of Uganda: Kanungu, where transmission is moderate, and Apac, where transmission is very high. Both gel and capillary methods evaluated polymorphic regions of the merozoite surface protein 1 and 2 and glutamine rich protein genes.
Results: Capillary electrophoresis detected more alleles and provided higher discriminatory power than agarose gel electrophoresis at both study sites. There was only moderate agreement between classification of outcomes with the two methods in Kanungu (kappa = 0.66) and poor agreement in Apac (kappa = 0.24). Overall efficacy results were similar when using gel vs. capillary methods in Kanungu (42-day risk of treatment failure for AL: 6.9% vs. 5.5%, p = 0.4; DP 2.4% vs. 2.9%, p = 0.5). However, the measured risk of recrudescence was significantly higher when using gel vs. capillary electrophoresis in Apac (risk of treatment failure for AL: 17.0% vs. 10.7%, p = 0.02; DP: 8.5% vs. 3.4%, p = 0.03). Risk differences between AL and DP were not significantly different whether gel or capillary methods were used.
Conclusions: Genotyping with gel electrophoresis overestimates the risk of recrudescence in anti-malarial trials performed in areas of high transmission intensity. Capillary electrophoresis provides more accurate outcomes for such trials and should be performed when possible. In areas of moderate transmission, gel electrophoresis appears adequate to estimate comparative risks of treatment failure.
Figures
References
-
- Greenhouse B, Dokomajilar C, Hubbard A, Rosenthal PJ, Dorsey G. Impact of transmission intensity on the accuracy of genotyping to distinguish recrudescence from new infection in antimalarial clinical trials. Antimicrob Agents Chemother. 2007;51:3096–3103. doi: 10.1128/AAC.00159-07. - DOI - PMC - PubMed
-
- Kamya MR, Yeka A, Bukirwa H, Lugemwa M, Rwakimari JB, Staedke SG, Talisuna AO, Greenhouse B, Nosten F, Rosenthal PJ, Wabwire-Mangen F, Dorsey G. Artemether-lumefantrine versus dihydroartemisinin-piperaquine for treatment of malaria: a randomized trial. PLoS Clin Trials. 2007;2:e20. doi: 10.1371/journal.pctr.0020020. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
