

Neuroradiological features of the tuberculosis-associated immune reconstitution inflammatory syndrome
- PMID: 20074410
- PMCID: PMC4176761
Neuroradiological features of the tuberculosis-associated immune reconstitution inflammatory syndrome
Abstract
Setting: Paradoxical tuberculosis-associated immune reconstitution inflammatory syndrome (TB-IRIS) is an important complication in human immunodeficiency virus type I (HIV-1) infected tuberculosis (TB) patients who start combination antiretroviral treatment (ART). Neurological manifestations occur in more than 10% of TB-IRIS cases. Apart from a few case reports, the radiological features of neurological TB-IRIS have not been described.
Objective: To describe the neuroradiological findings of patients with paradoxical neurological TB-IRIS.
Design: Computed tomography (CT; n = 13) and magnetic resonance imaging (n = 3) findings of 16 patients were reviewed.
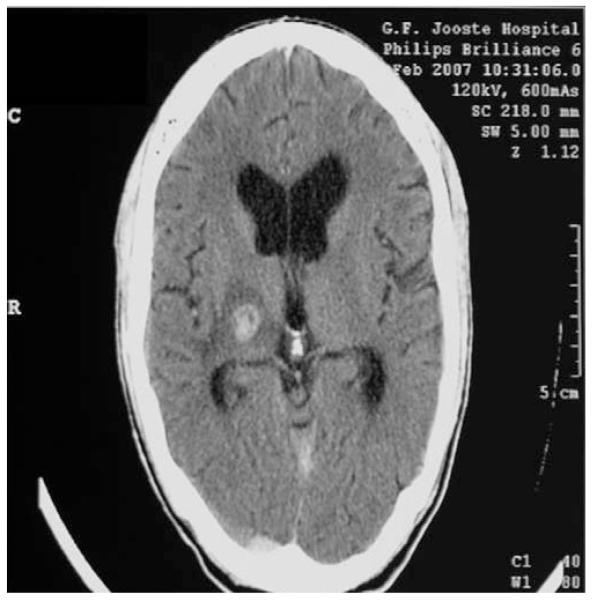
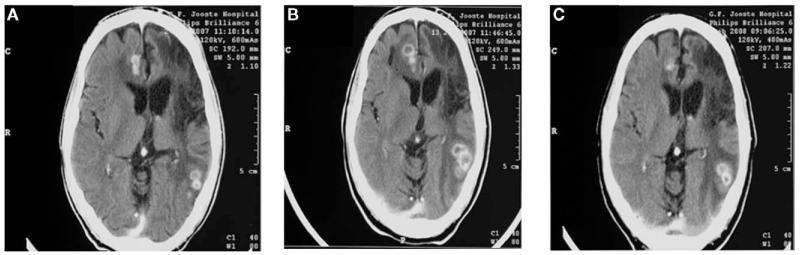
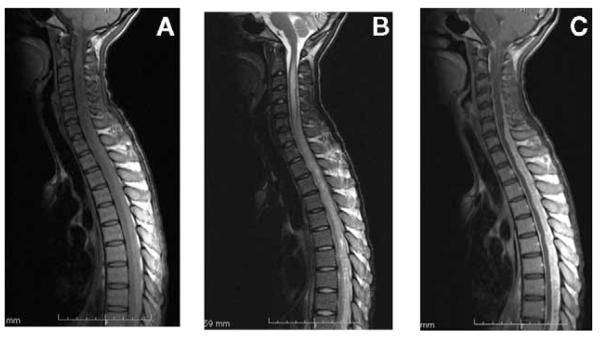
Results: IRIS manifestations included meningitis (n = 4), intracranial space occupying lesions (SOLs, presumed tuberculomas; n = 5), meningitis and SOLs (n = 5), radiculomyelitis (n = 1) and spondylitis (n = 1). In patients with tuberculoma IRIS, we observed a high prevalence of 1) low density lesions on non-contrast-enhanced CT (all lesions), 2) multiple lesions (in 5/10 patients) and 3) perilesional oedema (17/22 lesions). In patients with meningitis, meningeal enhancement (n = 2) and hydrocephalus (n = 1) were infrequently observed.
Conclusion: This is the first substantial series to describe the radiological features of paradoxical neurological TB-IRIS. Compared to published radiological findings of tuberculomas in HIV-1-infected patients (not receiving ART), an increased inflammatory response is suggested in tuberculoma IRIS. However, this was not observed in patients with TB meningitis IRIS.
Figures
Similar articles
-
Neurologic manifestations of paradoxical tuberculosis-associated immune reconstitution inflammatory syndrome: a case series.Clin Infect Dis. 2009 Jun 1;48(11):e96-107. doi: 10.1086/598988. Clin Infect Dis. 2009. PMID: 19405867
-
Paradoxical tuberculosis-associated immune reconstitution inflammatory syndrome in initiating ART among HIV-Infected patients in China-risk factors and management.BMC Infect Dis. 2024 Jan 2;24(1):5. doi: 10.1186/s12879-023-08897-3. BMC Infect Dis. 2024. PMID: 38166781 Free PMC article.
-
Neurological manifestations of TB-IRIS: a report of 4 children.Eur J Paediatr Neurol. 2012 Nov;16(6):676-82. doi: 10.1016/j.ejpn.2012.04.005. Epub 2012 May 30. Eur J Paediatr Neurol. 2012. PMID: 22658306
-
TB-IRIS pathogenesis and new strategies for intervention: Insights from related inflammatory disorders.Tuberculosis (Edinb). 2019 Sep;118:101863. doi: 10.1016/j.tube.2019.101863. Epub 2019 Sep 13. Tuberculosis (Edinb). 2019. PMID: 31561185 Review.
-
Central Nervous System Tuberculosis : Etiology, Clinical Manifestations and Neuroradiological Features.Clin Neuroradiol. 2019 Mar;29(1):3-18. doi: 10.1007/s00062-018-0726-9. Epub 2018 Sep 17. Clin Neuroradiol. 2019. PMID: 30225516 Review.
Cited by
-
Imaging spectrum of immunomodulating, chemotherapeutic and radiation therapy-related intracranial effects.Br J Radiol. 2018 Feb;91(1082):20170553. doi: 10.1259/bjr.20170553. Epub 2017 Nov 3. Br J Radiol. 2018. PMID: 29039692 Free PMC article. Review.
-
A systemic review of tuberculosis with HIV coinfection in children.Pediatr Radiol. 2017 Sep;47(10):1269-1276. doi: 10.1007/s00247-017-3895-9. Epub 2017 Aug 29. Pediatr Radiol. 2017. PMID: 29052773
-
A surgical case of cerebellar tuberculoma caused by a paradoxical reaction while on therapy for tuberculosis spondylitis.Surg Neurol Int. 2019 Aug 9;10:162. doi: 10.25259/SNI_318_2019. eCollection 2019. Surg Neurol Int. 2019. PMID: 31528497 Free PMC article.
-
Frequency, severity, and prediction of tuberculous meningitis immune reconstitution inflammatory syndrome.Clin Infect Dis. 2013 Feb;56(3):450-60. doi: 10.1093/cid/cis899. Epub 2012 Oct 24. Clin Infect Dis. 2013. PMID: 23097584 Free PMC article.
-
Ventriculoperitoneal shunt insertion for hydrocephalus in human immunodeficiency virus-infected adults: a systematic review and meta-analysis protocol.Syst Rev. 2017 Oct 16;6(1):201. doi: 10.1186/s13643-017-0603-7. Syst Rev. 2017. PMID: 29037257 Free PMC article.
References
-
- Corbett EL, Watt CJ, Walker N, et al. The growing burden of tuberculosis: global trends and interactions with the HIV epidemic. Arch Intern Med. 2003;163:1009–1021. - PubMed
-
- Badri M, Wilson D, Wood R. Effect of highly active antiretroviral therapy on incidence of tuberculosis in South Africa: a cohort study. Lancet. 2002;359:2059–2064. - PubMed
-
- Shelburne SA, III, Hamill RJ, Rodriguez-Barradas MC, et al. Immune reconstitution inflammatory syndrome: emergence of a unique syndrome during highly active antiretroviral therapy. Medicine. 2002;81:213–227. - PubMed
-
- Manosuthi W, Kiertiburanakul S, Phoorisri T, Sungkanuparph S. Immune reconstitution inflammatory syndrome of tuberculosis among HIV-infected patients receiving antituberculous and antiretroviral therapy. J Infect. 2006;53:357–363. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
