

Dissociation of obstructive sleep apnea from hypersomnolence and obesity in patients with stroke
- PMID: 20075361
- PMCID: PMC4230450
- DOI: 10.1161/STROKEAHA.109.566463
Dissociation of obstructive sleep apnea from hypersomnolence and obesity in patients with stroke
Abstract
Background and purpose: Obstructive sleep apnea (OSA) is seldom considered in the diagnostic investigation in the poststroke period although it is a stroke risk factor and has adverse prognostic implications after stroke. One reason might be that widely used clinical criteria for detection of OSA in the general community are not applicable in patients with stroke. We hypothesized that patients with stroke report less sleepiness and are less obese than subjects from a community sample with the same severity of OSA.
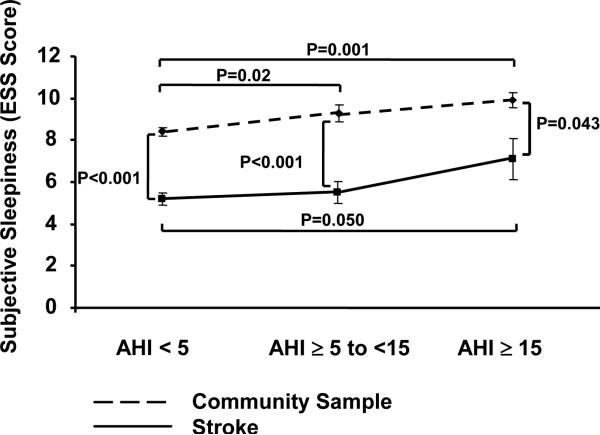
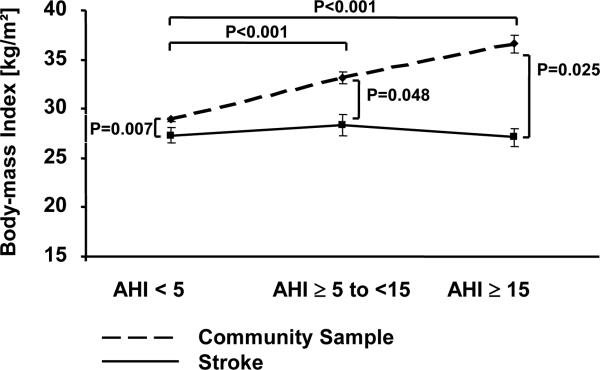
Methods: We performed polysomnography in 96 consecutive patients with stroke admitted to a stroke rehabilitation unit and in a community sample of 1093 subjects without a history of stroke. We compared the degrees of subjective sleepiness assessed by the Epworth Sleepiness Scale and body mass index between the 2 samples according to OSA categories assessed by the frequency of apneas and hypopneas per hour of sleep (<5, no OSA; 5 to <15 mild OSA; and >or=15, moderate to severe OSA).
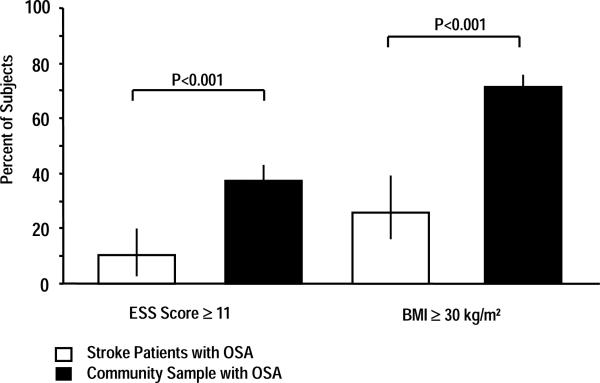
Results: Compared with the community sample, patients with stroke with OSA had significantly lower Epworth Sleepiness Scale scores and body mass index for mild OSA (Epworth Sleepiness Scale 9.3+/-0.3 versus 5.6+/-0.5, P<0.001 and body mass index 33.1+/-0.5 versus 28.5+/-1.1, P<0.048) and for moderate to severe OSA (Epworth Sleepiness Scale 9.7+/-0.4 versus 7.1+/-0.9, P=0.043 and body mass index 36.4+/-0.8 versus 27.2+/-0.8 kg/m(2), P<0.025).
Conclusions: For a given severity of OSA, patients with stroke had less daytime sleepiness and lower body mass index than subjects without stroke. These factors may make the diagnosis of OSA elusive in the poststroke period and preclude many such patients from the potential benefits of OSA therapy.
Figures
Similar articles
-
Subjective sleepiness and daytime functioning in bariatric patients with obstructive sleep apnea.Sleep Breath. 2013 Mar;17(1):267-74. doi: 10.1007/s11325-012-0685-3. Epub 2012 Apr 13. Sleep Breath. 2013. PMID: 22528950
-
Sleepiness and sleep in patients with both systolic heart failure and obstructive sleep apnea.Arch Intern Med. 2006 Sep 18;166(16):1716-22. doi: 10.1001/archinte.166.16.1716. Arch Intern Med. 2006. PMID: 16983049
-
The interaction between hypertension and obstructive sleep apnea on subjective daytime sleepiness.J Clin Hypertens (Greenwich). 2019 Mar;21(3):390-396. doi: 10.1111/jch.13485. Epub 2019 Feb 6. J Clin Hypertens (Greenwich). 2019. PMID: 30724462 Free PMC article.
-
The role of home sleep testing for evaluation of patients with excessive daytime sleepiness: focus on obstructive sleep apnea and narcolepsy.Sleep Med. 2019 Apr;56:80-89. doi: 10.1016/j.sleep.2019.01.014. Epub 2019 Jan 28. Sleep Med. 2019. PMID: 30803831 Review.
-
Investigation and management of residual sleepiness in CPAP-treated patients with obstructive sleep apnoea: the European view.Eur Respir Rev. 2022 May 25;31(164):210230. doi: 10.1183/16000617.0230-2021. Print 2022 Jun 30. Eur Respir Rev. 2022. PMID: 35613742 Free PMC article. Review.
Cited by
-
Association of sleep disordered breathing and cognitive deficit in APOE ε4 carriers.Sleep. 2013 Jun 1;36(6):873-80. doi: 10.5665/sleep.2714. Sleep. 2013. PMID: 23729930 Free PMC article.
-
Obstructive Sleep Apnea and Stroke: Determining the Mechanisms Behind their Association and Treatment Options.Transl Stroke Res. 2024 Apr;15(2):239-332. doi: 10.1007/s12975-023-01123-x. Epub 2023 Mar 16. Transl Stroke Res. 2024. PMID: 36922470 Review.
-
Novel and modifiable factors associated with adherence to continuous positive airway pressure therapy initiated during stroke rehabilitation: An exploratory analysis of a prospective cohort study.Sleep Med. 2022 Sep;97:43-46. doi: 10.1016/j.sleep.2022.05.013. Epub 2022 May 26. Sleep Med. 2022. PMID: 35716543 Free PMC article.
-
Prevalence, Effect on Functional Outcome, and Treatment of Sleep-Disordered Breathing in Patients With Subacute Stroke.J Clin Sleep Med. 2019 Jun 15;15(6):891-897. doi: 10.5664/jcsm.7844. J Clin Sleep Med. 2019. PMID: 31138390 Free PMC article.
-
Sleep-related symptoms in patients with mild stroke.J Clin Sleep Med. 2020 Jan 15;16(1):55-64. doi: 10.5664/jcsm.8122. Epub 2019 Dec 4. J Clin Sleep Med. 2020. PMID: 31957653 Free PMC article.
References
-
- Munoz R, Duran-Cantolla J, Martinez-Vila E, Gallego J, Rubio R, Aizpuru F, De La Torre G. Severe sleep apnea and risk of ischemic stroke in the elderly. Stroke. 2006;37:2317–2321. - PubMed
-
- Becker HF, Jerrentrup A, Ploch T, Grote L, Penzel T, Sullivan CE, Peter JH. Effect of nasal continuous positive airway pressure treatment on blood pressure in patients with obstructive sleep apnea. Circulation. 2003;107:68–73. - PubMed
-
- Punjabi NM, Sorkin JD, Katzel LI, Goldberg AP, Schwartz AR, Smith PL. Sleep-disordered breathing and insulin resistance in middle-aged and overweight men. Am J Respir Crit Care Med. 2002;165:677–682. - PubMed
-
- Martinez-Garcia MA, Soler-Cataluna JJ, Ejarque-Martinez L, Soriano Y, Roman-Sanchez P, Barbe Illa F, Montserrat Canal JM, Duran-Cantolla J. CPAP treatment reduces mortality in ischemic stroke patients with obstructive sleep apnea. Am J Respir Crit Care Med. 2009 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
