

Femoral shortening in total hip arthroplasty for high developmental dysplasia of the hip
- PMID: 20077043
- PMCID: PMC2881990
- DOI: 10.1007/s11999-009-1218-7
Femoral shortening in total hip arthroplasty for high developmental dysplasia of the hip
Abstract
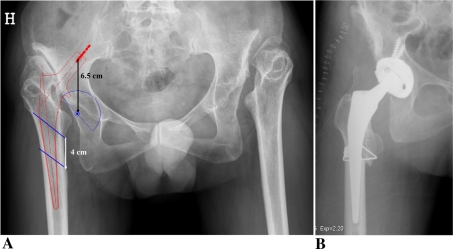
Background: When reconstructing a hip with developmental dysplasia with a high dislocation, placing the acetabular component in the anatomic position can result in a prosthetic hip that is difficult to reduce. Subtrochanteric femoral osteotomy and shortening makes reduction easier but can be associated with complications (eg, limp, sciatic nerve injury, nonunion of the osteotomy) or compromise long-term stem survival.
Questions/purposes: We therefore evaluated (1) the short-term complication rate, (2) functional scores, and (3) survivorship of prostheses in patients with high developmental dysplasia of the hip reconstructed with femoral shortening.
Patients and methods: We prospectively followed 46 patients (65 hips) operated on from 1990 to 2000. There were 34 females and 12 males with a mean age of 48 years (range, 16-79 years). Before surgery, all patients had a positive Trendelenburg test. The minimum followup was 8 years (mean, 13 years; range, 8-18 years).
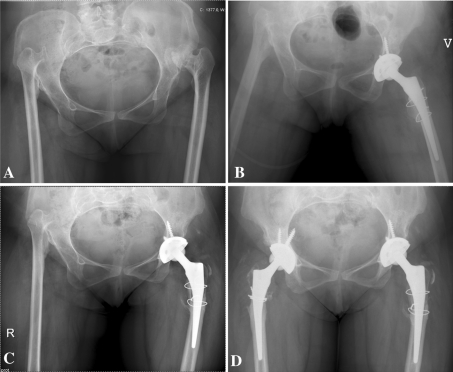
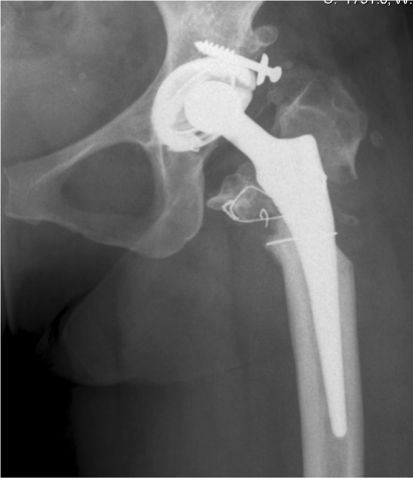
Results: One patient experienced recurrent dislocation and two peroneal nerve palsies, one of which partially recovered and one of which was permanent. In one patient, the stem subsided and after 8 months was replaced by a larger stem that stabilized. One patient had a nonunion but was functioning well and did not have additional surgery. At followup, 12 of the 65 hips (18%) had a positive Trendelenburg test. The mean muscle strength of the abductors was 4 (range, 3-5). The mean Harris hip score was 87 (range, 59-100) and the mean visual analog scale pain score 81 (range, 35-100). At followup, all stems were well fixed with no obvious signs of radiographic loosening. Ten cups were revised because of aseptic loosening.
Conclusions: Our data suggest femoral osteotomy and shortening at the subtrochanteric level predictably allows a stable reduction in patients with high developmental dysplasia of the hip and does not lead to any reduction in long-term survival.
Level of evidence: Level II, prognostic study. See Guidelines for Authors for a complete description of levels of evidence.
Figures
References
-
- Argenson JN, Flecher X, Parratte S, Aubaniac JM. Anatomy of the dysplastic hip and consequences for total hip arthroplasty. Clin Orthop Relat Res. 2007;465:40–45. - PubMed
-
- Callaghan JJ, Forest EE, Sporer SM, Goetz DD, Johnston RC. Total hip arthroplasty in the young adult. Clin Orthop Relat Res. 1997;344:257–262. - PubMed
-
- DeLee JG, Charnley J. Radiological demarcation of cemented sockets in total hip replacement. Clin Orthop Relat Res. 1976;121:20–32. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
