

Quantitative pharmacology approach in Alzheimer's disease: efficacy modeling of early clinical data to predict clinical outcome of tesofensine
- PMID: 20077053
- PMCID: PMC2844519
- DOI: 10.1208/s12248-009-9164-6
Quantitative pharmacology approach in Alzheimer's disease: efficacy modeling of early clinical data to predict clinical outcome of tesofensine
Abstract
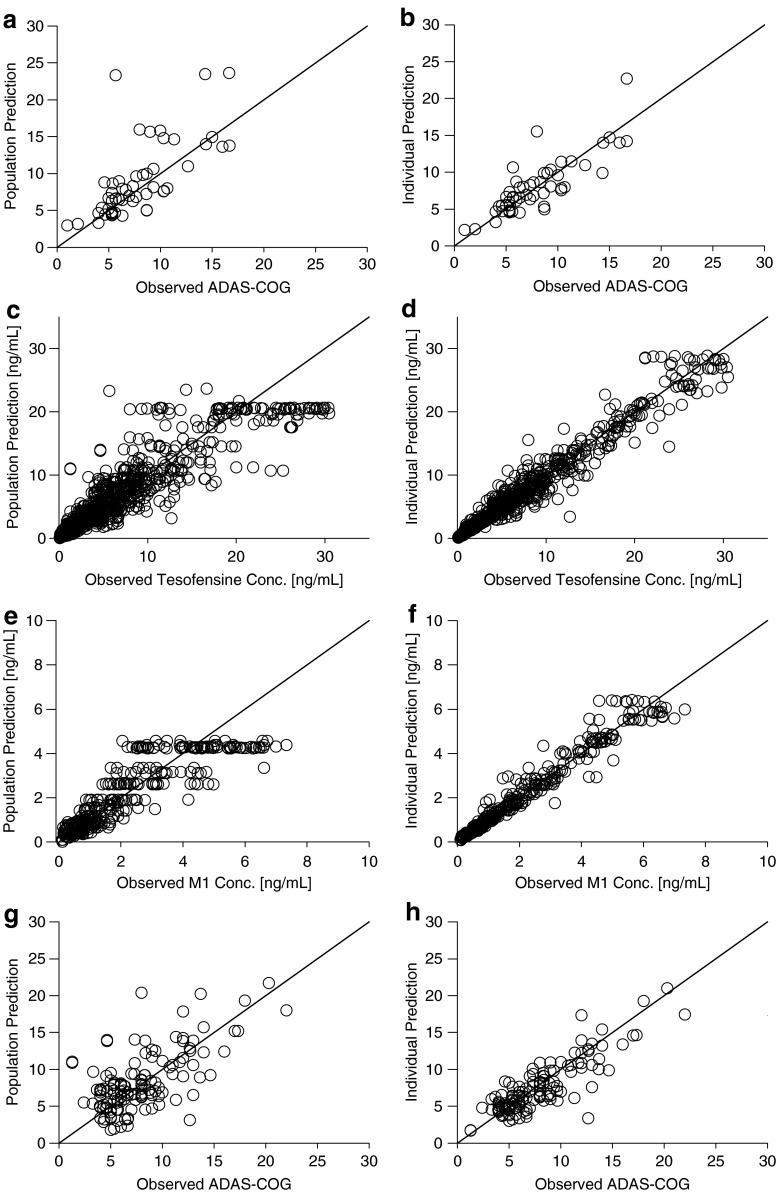
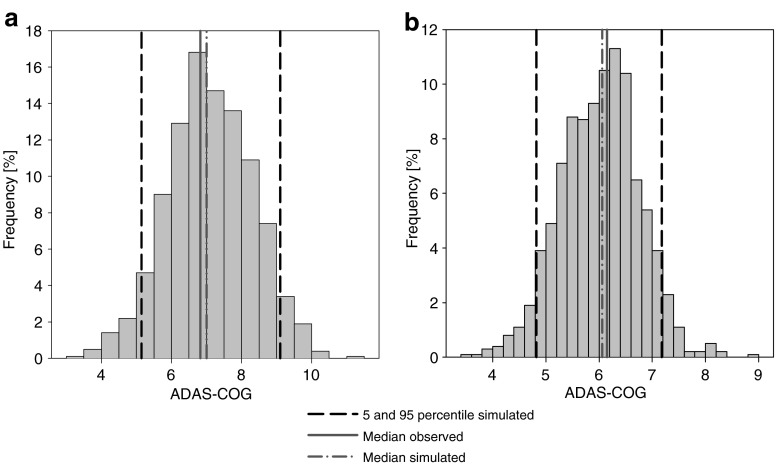
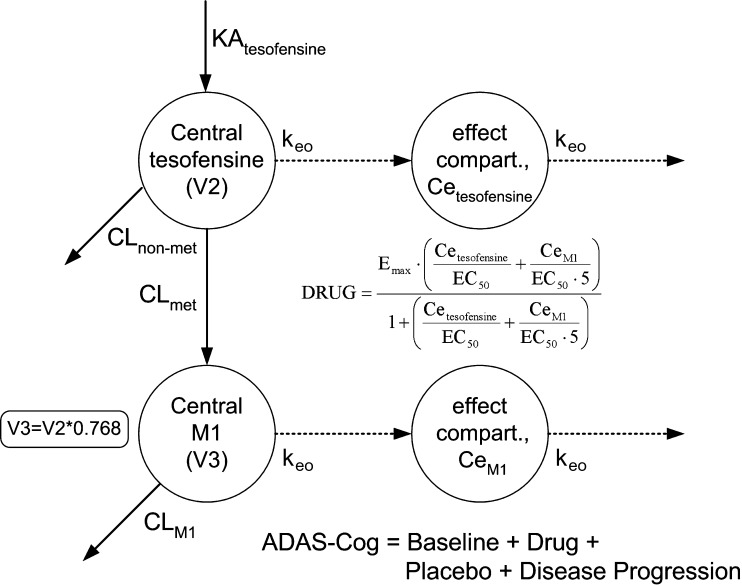
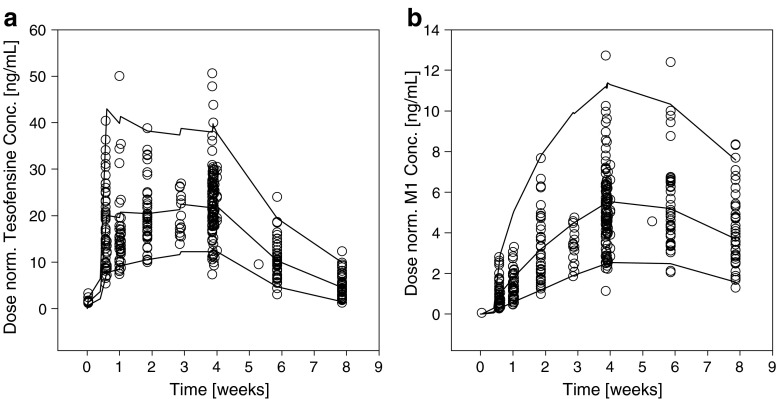
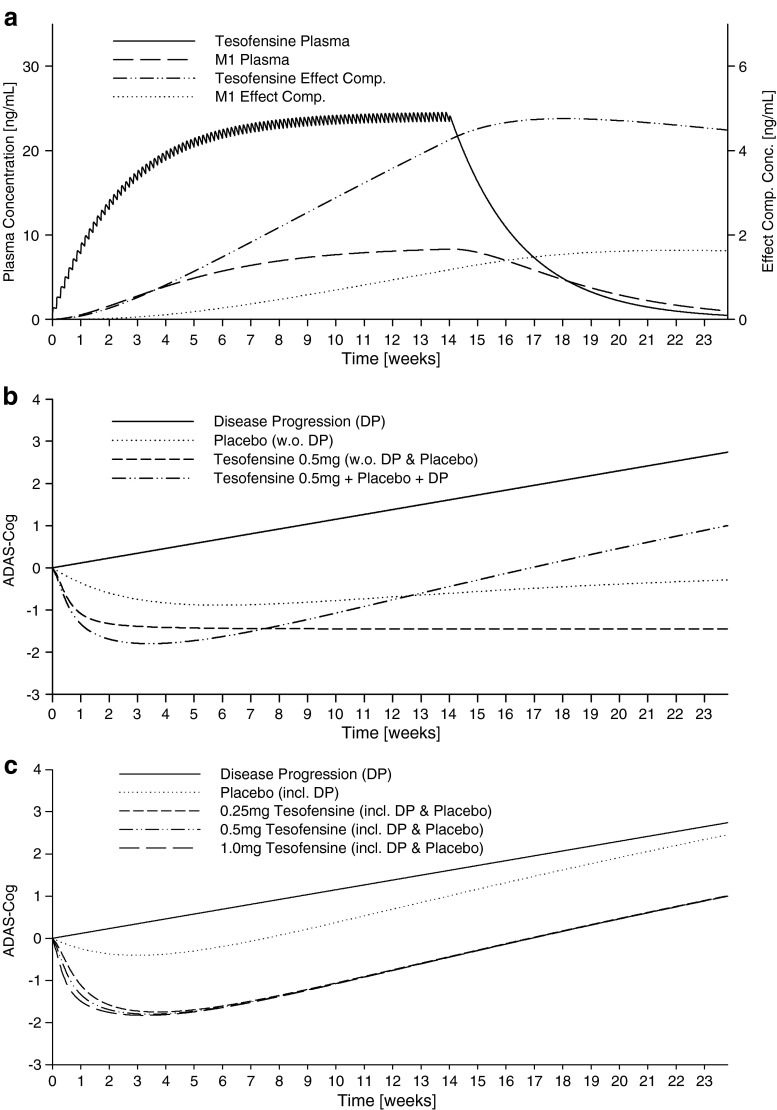
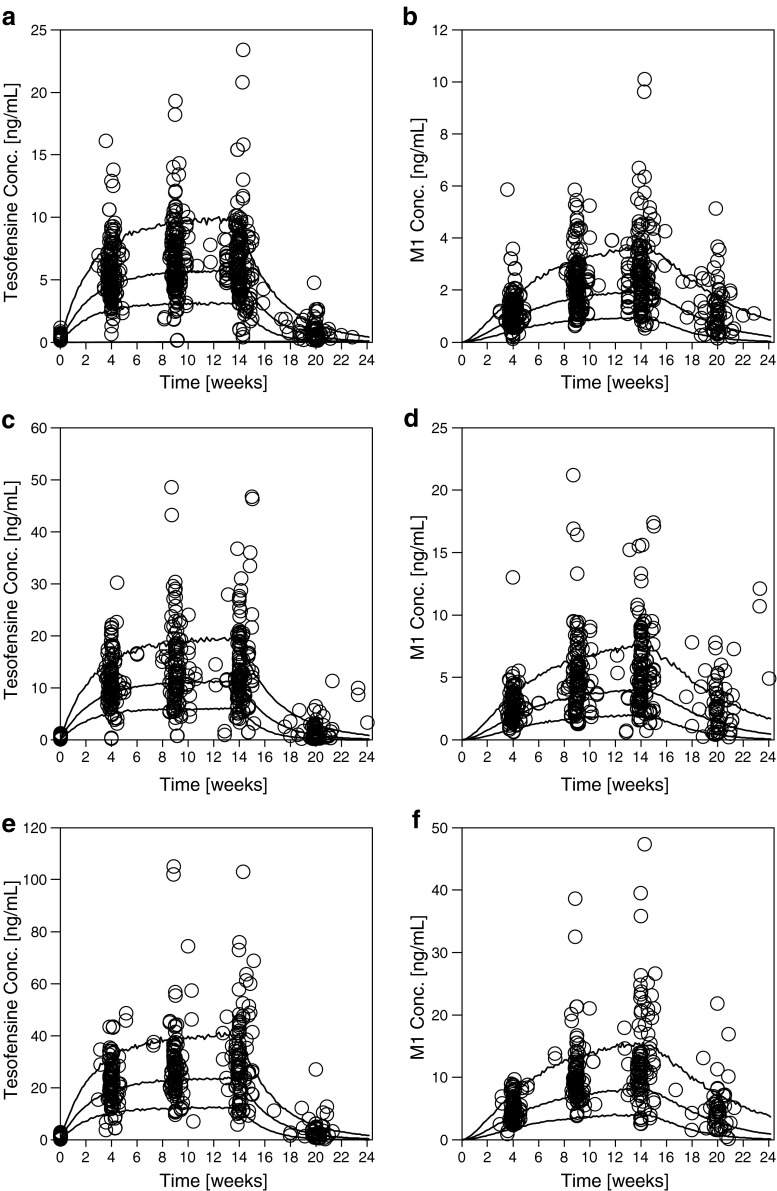
Effective therapeutic options for Alzheimer's disease (AD) are limited and much research is currently ongoing. The high attrition rate in drug development is a critical issue. Here, the quantitative pharmacology approach (QP-A) and model-based drug development (MBDD) provide a valuable opportunity to support early selection of the most promising compound and facilitate a fast, efficient, and rational drug development process. The aim of this analysis was to exemplify the QP-A by eventually predicting the clinical outcome of a proof-of-concept (PoC) trial of tesofensine in AD patients from two small phase IIa trials. Retrospective population pharmacokinetic/pharmacodynamic (PK/PD) modeling of tesofensine, its metabolite M1, and assessment scale-cognitive subscale data from two 4-week placebo-controlled studies in 62 mild AD patients was performed using non-linear mixed effects modeling. The final PK/PD model was used to predict data of a negative 14-week phase IIb PoC trial (430 AD patients). For the PK, one-compartment models for tesofensine and M1 with first-order absorption and elimination were sufficient. An extended Emax model including disease progression best described the PK/PD relationship using effect compartments. The placebo effect was also implemented in the final PK/PD model based on a published placebo model developed in a large AD cohort. Various internal evaluation techniques confirmed the reliability and predictive performance of the PK/PD model, which also successfully predicted the 14-week PoC data. For tesofensine, the dose concentration-effect relationship has successfully been described in mild AD patients demonstrating the supportive value of PK/PD models in QP-A/MBDD in early phases of clinical development for decision-making.
Figures


References
-
- Tufts Center for the Study of Drug Development. Impact Report: Fastest drug developers consistently best peers on key performance metrics, Tufts University, Boston, 2006.
-
- US Food and Drug Administration. Innovation or Stagnation: Challenge and opportunity on the critical path to new medical products, Rockville, 2004.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
