

Advances in diagnosing and managing antibody-mediated rejection
- PMID: 20077121
- PMCID: PMC2923704
- DOI: 10.1007/s00467-009-1386-4
Advances in diagnosing and managing antibody-mediated rejection
Abstract
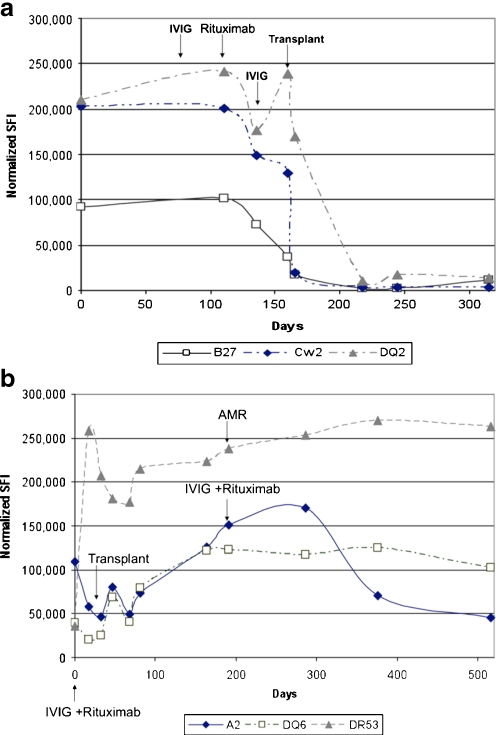
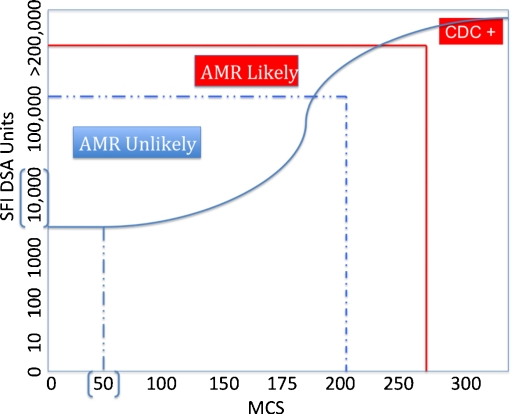
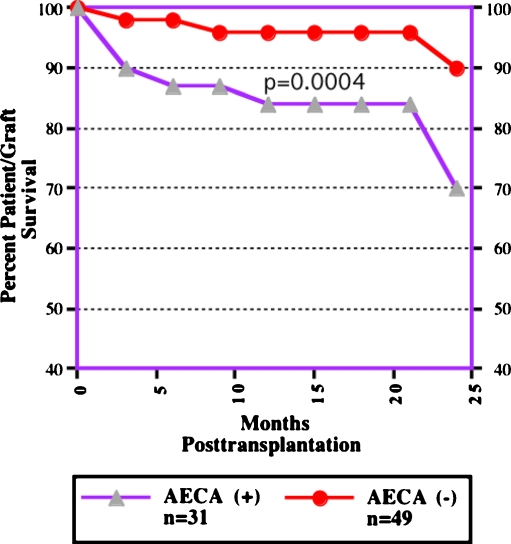
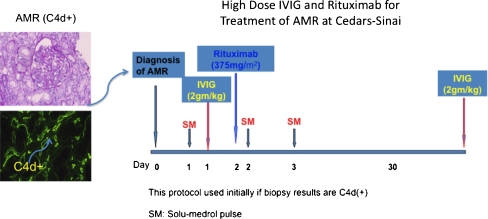
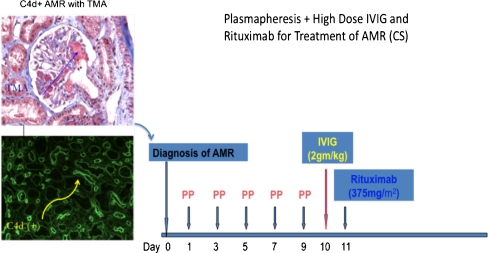
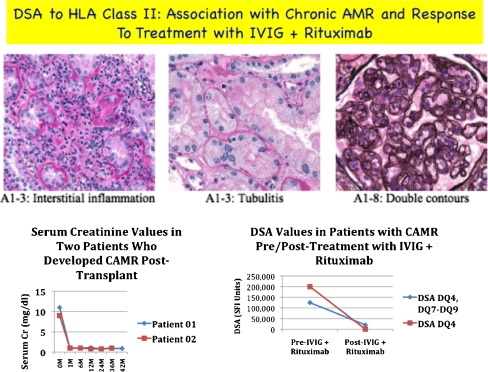
Antibody-mediated rejection (AMR) is a unique, significant, and often severe form of allograft rejection that is not amenable to treatment with standard immunosuppressive medications. Significant advances have occurred in our ability to predict patients at risk for, and to diagnose, AMR. These advances include the development of newer anti-human leukocyte antigen (HLA)-antibody detection techniques and assays for non-HLA antibodies associated with AMR. The pathophysiology of AMR suggests a prime role for antibodies, B cells and plasma cells, but other effector molecules, especially the complement system, point to potential targets that could modify the AMR process. An emerging and potentially larger problem is the development of chronic AMR (CAMR) resulting from de novo donor-specific anti-HLA antibodies (DSA) that emerge more than 100 days posttransplantation. Therapeutic options include: (1) High-dose intravenously administered immunoglobulin (IVIG), which has many potential benefits. (2) The use of IVIG+rituximab (anti-CD20, anti-B cell). (3) The combination of plasmapheresis (PP)+low-dose IVIG with or without rituximab. Data support the efficacy of all of the above approaches. Newer approaches to treating AMR include using the proteosome inhibitor (bortezomib), which induces apoptosis in plasma cells, and eculizumab (anti-C5, anticomplement monoclonal antibody).
Figures
Similar articles
-
Treatment of Biopsy-Proven Acute Antibody-Mediated Rejection Using Thymoglobulin (ATG) Monotherapy and a Combination of Rituximab, Intravenous Immunoglobulin, and Plasmapheresis: Lesson Learned from Primary Experience.Clin Transpl. 2014:223-30. Clin Transpl. 2014. PMID: 26281149
-
Combination of Total Lymphoid Irradiation, Low-Dose IVIG and ATG as Rescue Therapy for Highly Sensitized and Antibody-Mediated Rejection Renal Transplant Recipients.Clin Transpl. 2014:215-21. Clin Transpl. 2014. PMID: 26281148 Clinical Trial.
-
Frequent development of subclinical chronic antibody-mediated rejection within 1 year after renal transplantation with pre-transplant positive donor-specific antibodies and negative CDC crossmatches.Hum Immunol. 2013 Sep;74(9):1111-8. doi: 10.1016/j.humimm.2013.06.022. Epub 2013 Jun 18. Hum Immunol. 2013. PMID: 23792054
-
Antibody-mediated rejection: treatment alternatives and outcomes.Transplant Rev (Orlando). 2009 Jan;23(1):34-46. doi: 10.1016/j.trre.2008.08.004. Transplant Rev (Orlando). 2009. PMID: 19027615 Review.
-
Deciphering antibody-mediated rejection: new insights into mechanisms and treatment.Curr Opin Organ Transplant. 2010 Feb;15(1):8-10. doi: 10.1097/MOT.0b013e3283342712. Curr Opin Organ Transplant. 2010. PMID: 19890210 Review.
Cited by
-
Acute antibody-mediated rejection in paediatric renal transplant recipients.Pediatr Nephrol. 2011 Jul;26(7):1149-56. doi: 10.1007/s00467-011-1864-3. Epub 2011 Apr 1. Pediatr Nephrol. 2011. PMID: 21461632
-
Anti-Human Leukocyte Antigen Antibody Detection from Terasaki's Humoral Theory to Delisting Strategies in 2024.Int J Mol Sci. 2025 Jan 13;26(2):630. doi: 10.3390/ijms26020630. Int J Mol Sci. 2025. PMID: 39859344 Free PMC article. Review.
-
The paradoxical functions of B cells and antibodies in transplantation.J Immunol. 2013 Feb 1;190(3):875-9. doi: 10.4049/jimmunol.1100120. J Immunol. 2013. PMID: 23335803 Free PMC article. Review.
-
Therapeutic plasma exchange for the treatment of pediatric renal diseases in 2013.Pediatr Nephrol. 2014 Jan;29(1):35-50. doi: 10.1007/s00467-013-2479-7. Epub 2013 Jun 29. Pediatr Nephrol. 2014. PMID: 23812351 Review.
-
Evaluation of Cumulative Effect of Standard Triple Immunosuppression on Prevention of De Novo Donor Specific Antibodies (dnDSA) Production in Children after Kidney Transplantation-A Retrospective and Prospective Study.Children (Basel). 2021 Dec 9;8(12):1162. doi: 10.3390/children8121162. Children (Basel). 2021. PMID: 34943360 Free PMC article.
References
-
- Organ Procurement Transplantation Network/Scientific Registry of Transplant Recipients: OPTN. (2009); http://www.optn.org/data/ - PubMed
-
- United Network for Organ Sharing Data Base as of 5/30/2008. http://www.unos.org
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
