

Advances in diagnosing and managing antibody-mediated rejection
- PMID: 20077121
- PMCID: PMC2923704
- DOI: 10.1007/s00467-009-1386-4
Advances in diagnosing and managing antibody-mediated rejection
Abstract
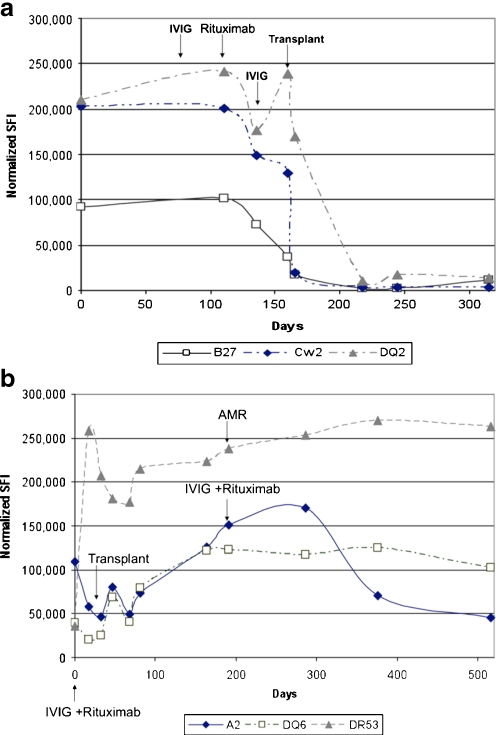
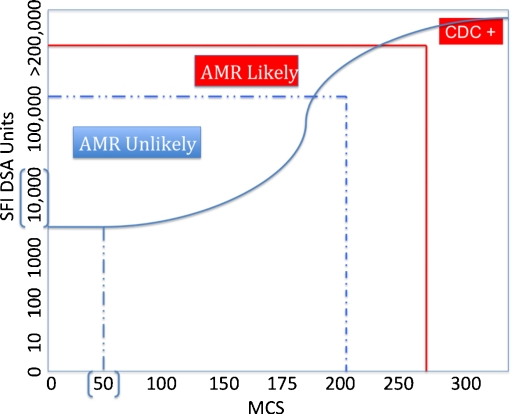
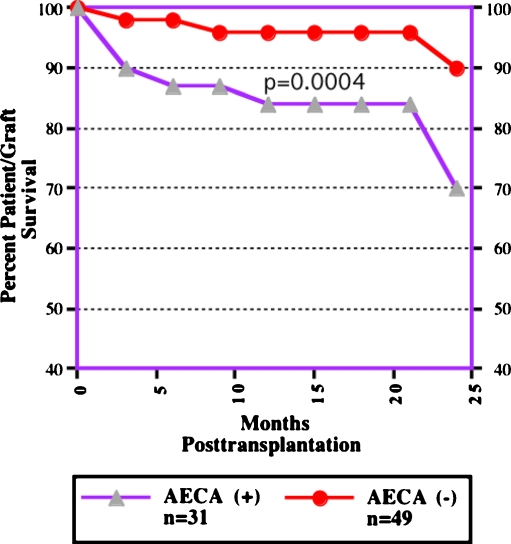
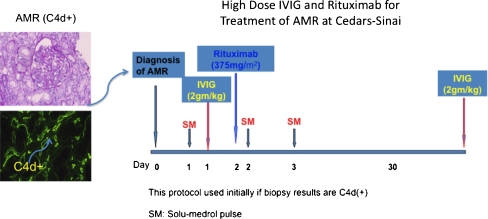
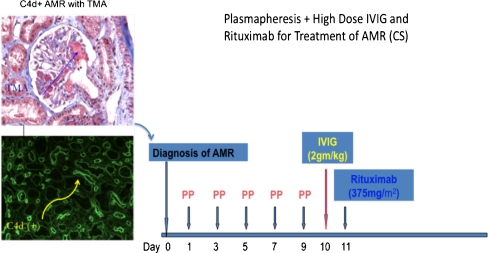
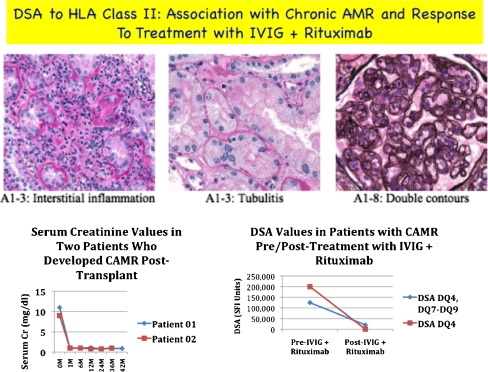
Antibody-mediated rejection (AMR) is a unique, significant, and often severe form of allograft rejection that is not amenable to treatment with standard immunosuppressive medications. Significant advances have occurred in our ability to predict patients at risk for, and to diagnose, AMR. These advances include the development of newer anti-human leukocyte antigen (HLA)-antibody detection techniques and assays for non-HLA antibodies associated with AMR. The pathophysiology of AMR suggests a prime role for antibodies, B cells and plasma cells, but other effector molecules, especially the complement system, point to potential targets that could modify the AMR process. An emerging and potentially larger problem is the development of chronic AMR (CAMR) resulting from de novo donor-specific anti-HLA antibodies (DSA) that emerge more than 100 days posttransplantation. Therapeutic options include: (1) High-dose intravenously administered immunoglobulin (IVIG), which has many potential benefits. (2) The use of IVIG+rituximab (anti-CD20, anti-B cell). (3) The combination of plasmapheresis (PP)+low-dose IVIG with or without rituximab. Data support the efficacy of all of the above approaches. Newer approaches to treating AMR include using the proteosome inhibitor (bortezomib), which induces apoptosis in plasma cells, and eculizumab (anti-C5, anticomplement monoclonal antibody).
Figures
References
-
- Organ Procurement Transplantation Network/Scientific Registry of Transplant Recipients: OPTN. (2009); http://www.optn.org/data/ - PubMed
-
- United Network for Organ Sharing Data Base as of 5/30/2008. http://www.unos.org
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
