

Self-management rehabilitation and health-related quality of life in Parkinson's disease: a randomized controlled trial
- PMID: 20077478
- PMCID: PMC2831132
- DOI: 10.1002/mds.22940
Self-management rehabilitation and health-related quality of life in Parkinson's disease: a randomized controlled trial
Abstract
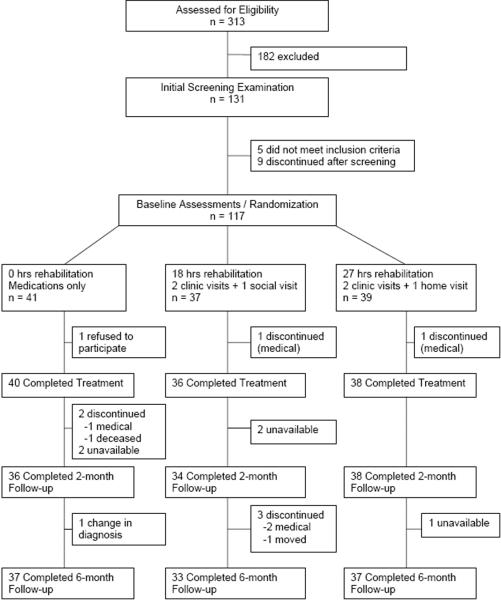
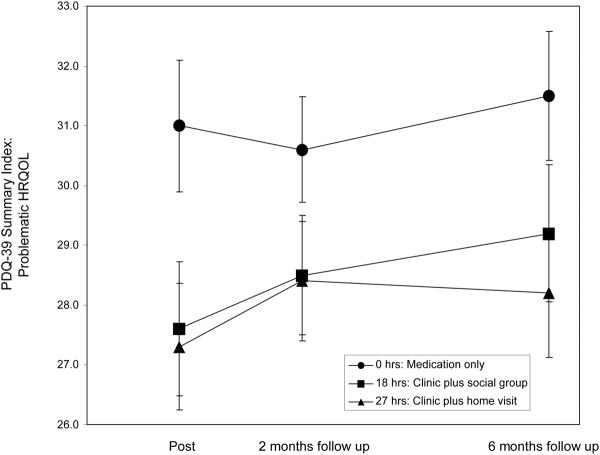
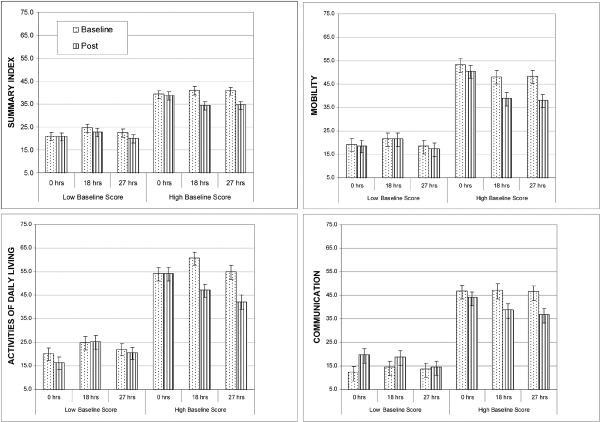
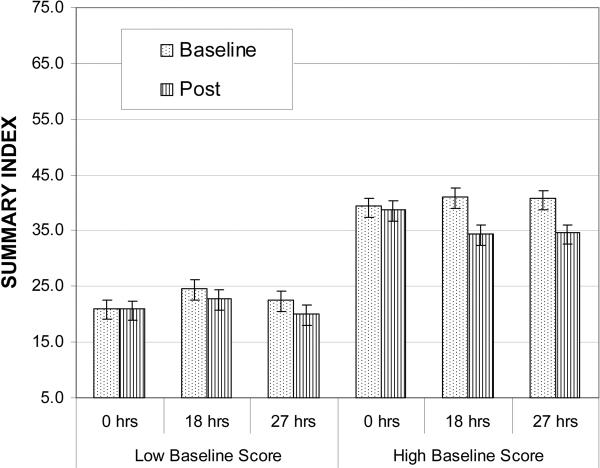
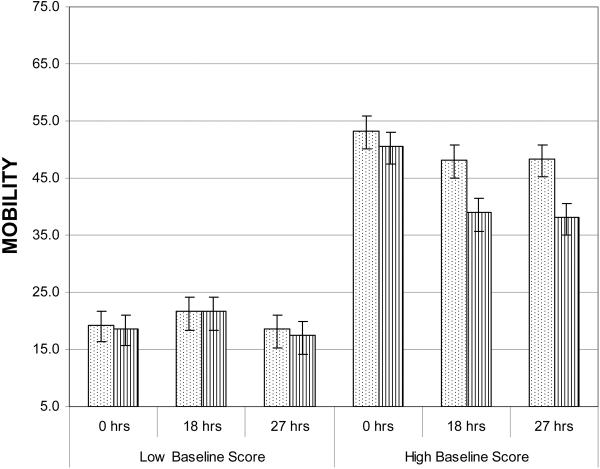
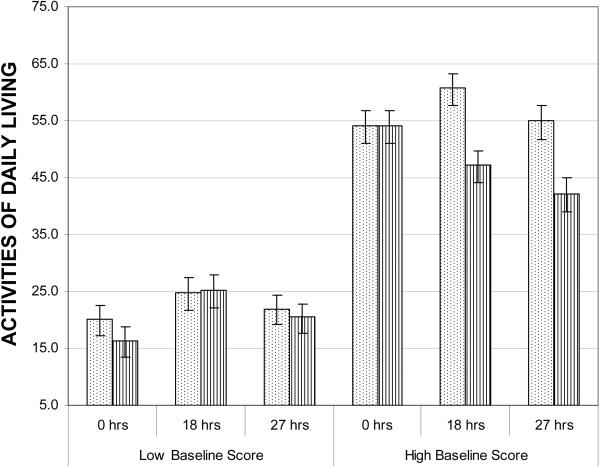
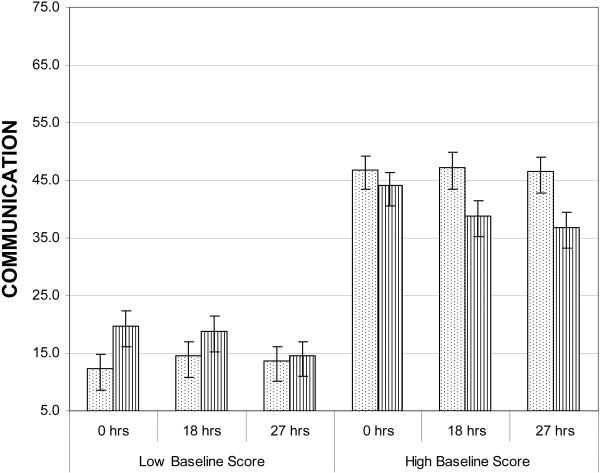
The purpose of this randomized controlled trial was to determine whether increasing hours of self-management rehabilitation had increasing benefits for health-related quality of life (HRQOL) in Parkinson's disease beyond best medical treatment, whether effects persisted at 2 and 6 months of follow-up, and whether targeted compared with nontargeted HRQOL domains responded more to rehabilitation. Participants on best medication therapy were randomly assigned to one of three conditions for 6 weeks intervention: 0 hours of rehabilitation; 18 hours of clinic group rehabilitation plus 9 hours of attention control social sessions; and 27 hours of rehabilitation, with 18 in clinic group rehabilitation and 9 hours of rehabilitation designed to transfer clinic training into home and community routines. Results (N = 116) showed that at 6 weeks, there was a beneficial effect of increased rehabilitation hours on HRQOL measured with the Parkinson's Disease Questionnaire-39 summary index (F(1,112) = 6.48, eta = 0.23, CI = 0.05-0.40, P = 0.01). Benefits persisted at follow-up. The difference between 18 and 27 hours was not significant. Clinically relevant improvement occurred at a greater rate for 18 and 27 hours (54% improved) than for 0 hours (18% improved), a significant 36% difference in rates (95% CI = 20-52% difference). Effects were largest in two targeted domains: communication and mobility. More concerns with mobility and activities of daily living at baseline predicted more benefit from rehabilitation.
(c) 2010 Movement Disorder Society.
Figures
References
-
- Den Oudsten BL, Van Heck GL, De Vries J. Quality of life and related concepts in Parkinson's disease: a systematic review. Mov Disord. 2007;22:1528–1537. - PubMed
-
- Holroyd S, Currie LJ, Wooten GF. Depression is associated with impairment of ADL, not motor function in Parkinson disease. Neurology. 2005;64:2134–2135. - PubMed
-
- Livneh H, Antonak RF. Review of research on psychosocial adaptation to neuromuscular disorders: I. Cerebral Palsy, Muscular Dystrophy, and Parkinson's Disease. J Soc Behav Pers. 1994;9:201–230.
-
- Koplas PA, Gans HB, Wisely MP, et al. Quality of life and Parkinson's disease. J Gerontol A Biol Sci Med Sci. 1999;54:M197–M202. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
