

Sarcoplasmic reticulum Ca(2+) ATPase as a therapeutic target for heart failure
- PMID: 20078230
- PMCID: PMC3001226
- DOI: 10.1517/14712590903321462
Sarcoplasmic reticulum Ca(2+) ATPase as a therapeutic target for heart failure
Abstract
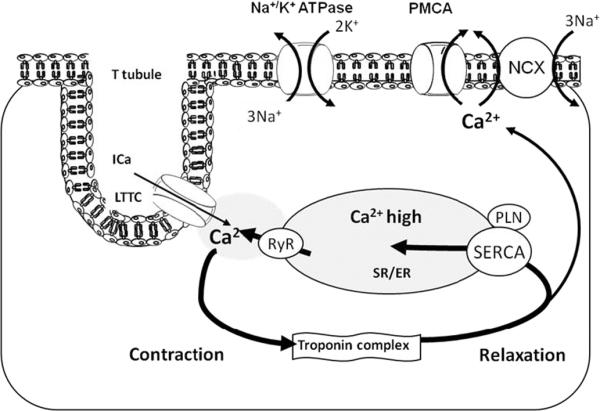
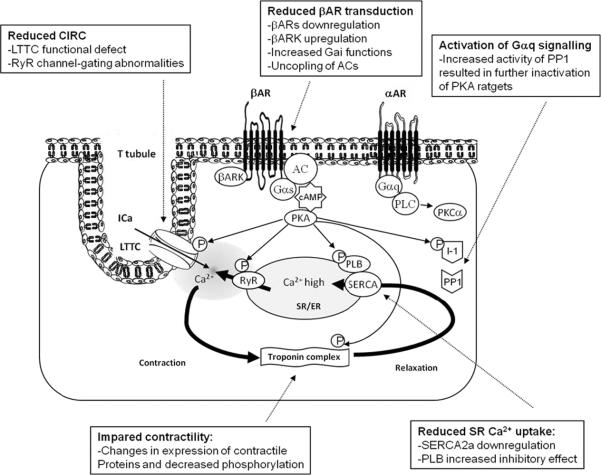
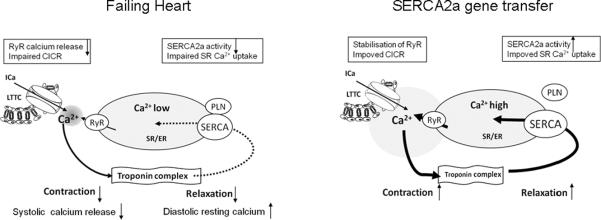
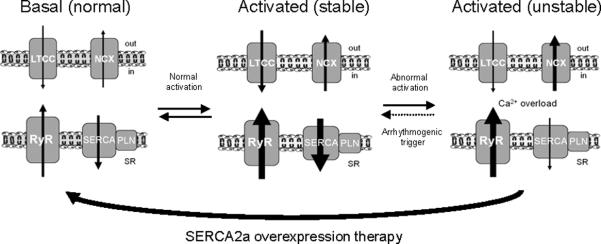
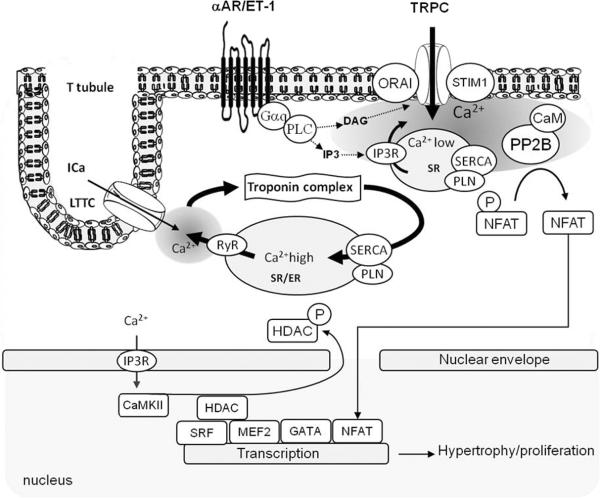
The cardiac isoform of the sarco/endoplasmic reticulum Ca(2+)ATPase (SERCA2a) plays a major role in controlling excitation/contraction coupling. In both experimental and clinical heart failure, SERCA2a expression is significantly reduced which leads to abnormal Ca(2+) handling and deficient contractility. A large number of studies in isolated cardiac myocytes and in small and large animal models of heart failure showed that restoring SERCA2a expression by gene transfer corrects the contractile abnormalities and improves energetics and electrical remodeling. Following a long line of investigation, a clinical trial is underway to restore SERCA2a expression in patients with heart failure using adeno-associated virus type 1. This review addresses the following issues regarding heart failure gene therapy: i) new insights on calcium regulation by SERCA2a; ii) SERCA2a as a gene therapy target in animal models of heart failure; iii) advances in the development of viral vectors and gene delivery; and iv) clinical trials on heart failure using SERCA2a. This review focuses on the new advances in SERCA2a- targeted gene therapy made in the last three years. In conclusion, SERCA2a is an important therapeutic target in various cardiovascular disorders. Ongoing clinical gene therapy trials will provide answers on its safety and applicability.
Figures
References
-
- Rosamond W, Flegal K, Furie K, Go A, Greenlund K, Haase N, et al. Heart disease and stroke statistics--2008 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2008 Jan 29;117(4):e25–146. - PubMed
-
- Jessup M, Brozena S. Heart failure. N Engl J Med. 2003 May 15;348(20):2007–18. - PubMed
-
- Lipskaia L, Ly H, Kawase Y, Hajjar R, Lompre AM. Treatment of heart failure by calcium cycling gene therapy. Future Cardiology. 2007;3(4):413–23. - PubMed
-
- Del Monte F, Hajjar RJ. Intracellular devastation in heart failure. Heart Fail Rev. 2008 Jun;13(2):151–62. - PubMed
-
- Kawase Y, Hajjar RJ. The cardiac sarcoplasmic/endoplasmic reticulum calcium ATPase: a potent target for cardiovascular diseases. Nat Clin Pract Cardiovasc Med. 2008 Sep;5(9):554–65. - PubMed
-
**Review on calcum cycling gene therapy
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous