

Corticosteroids correct aberrant CFTR localization in the duct and regenerate acinar cells in autoimmune pancreatitis
- PMID: 20080093
- PMCID: PMC3061436
- DOI: 10.1053/j.gastro.2010.01.001
Corticosteroids correct aberrant CFTR localization in the duct and regenerate acinar cells in autoimmune pancreatitis
Abstract
Background & aims: Corticosteroids are now widely accepted as a treatment for autoimmune pancreatitis (AIP). However, the molecular mechanism by which steroid treatment improves AIP remains largely unknown. The aim of this study was to elucidate cellular mechanisms by which corticosteroids improve both pancreatic exocrine function and histopathology in AIP.
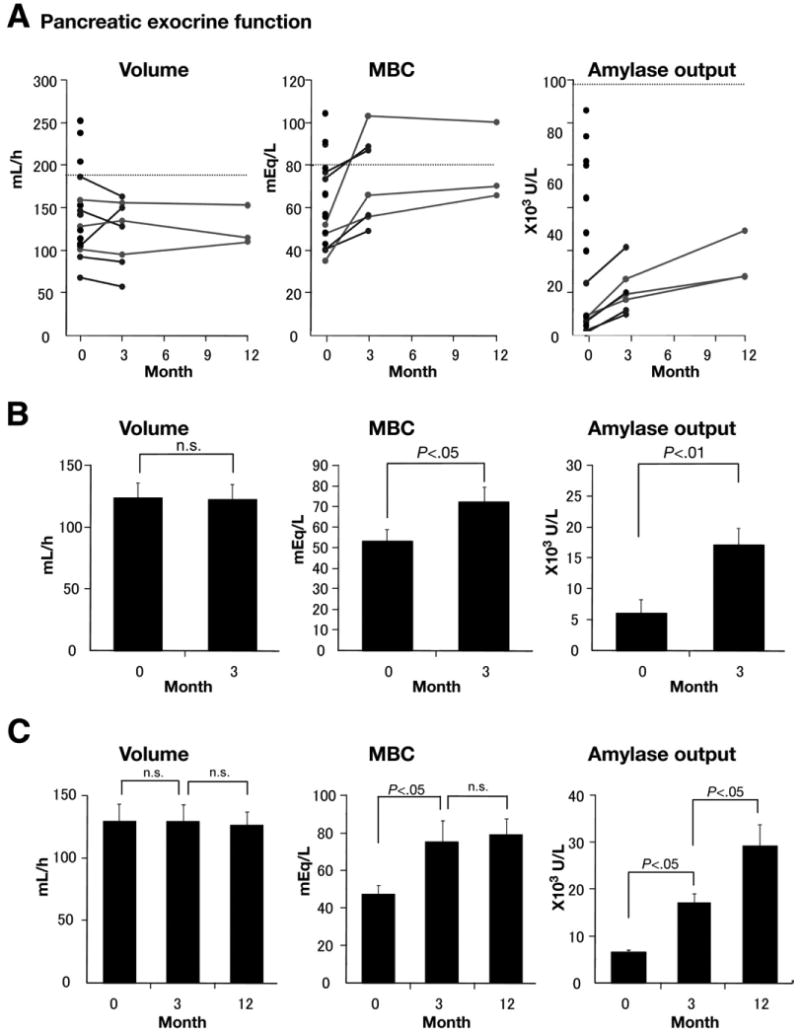
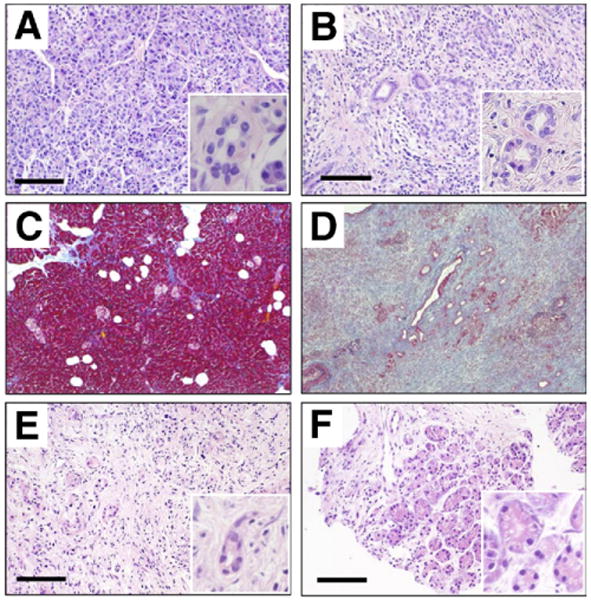
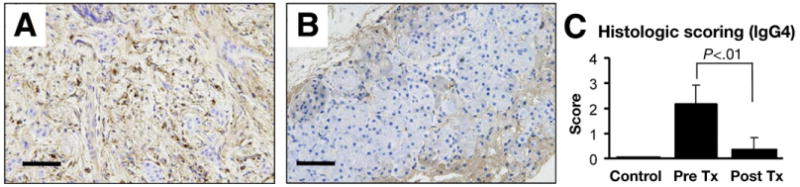
Methods: Pancreatic exocrine function was evaluated by the secretin-stimulated function test and pancreatic biopsy specimens were processed for histologic analysis at the time of diagnosis and 3 months after initiation of steroid treatment. Expression and localization of proteins was assayed by immunohistochemistry. Analysis of immunoglobulin (Ig)G4-positive plasma cells was used to verify inflammation in AIP.
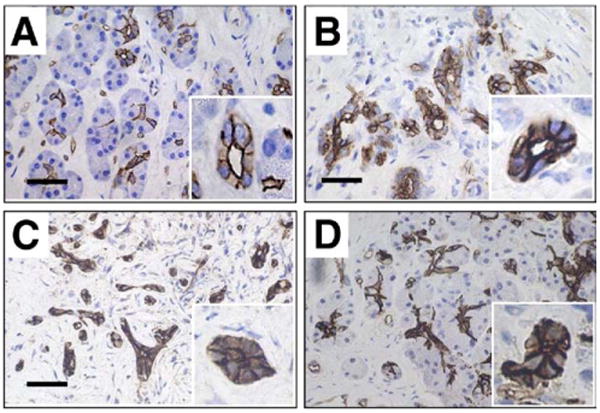
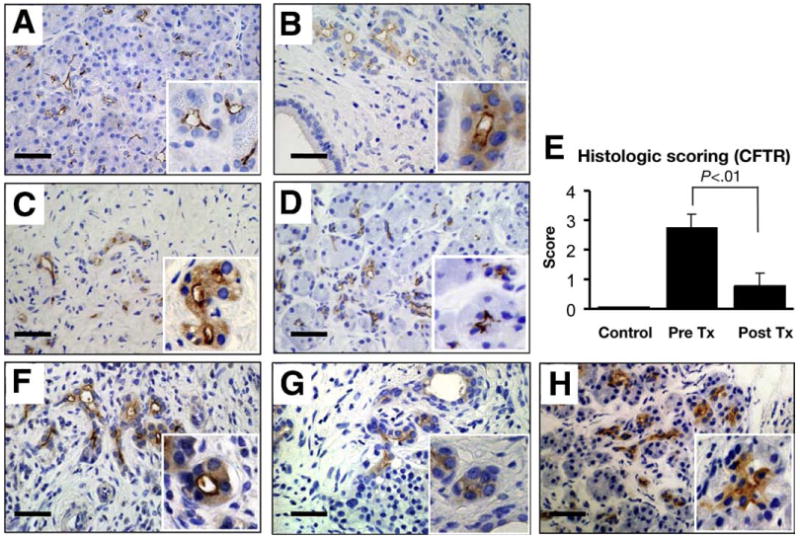
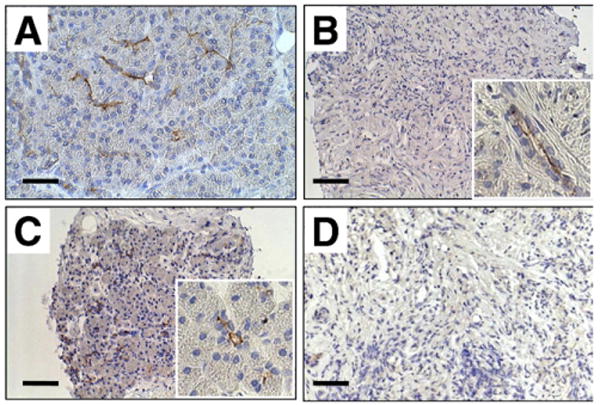
Results: The number of IgG4-positive plasma cells in pancreatic sections was decreased by steroid treatment, indicating reduced inflammation. Fluid, bicarbonate (HCO(3)(-)), and digestive enzyme secretions all were impaired in most patients with AIP. Corticosteroids improved both HCO(3)(-) and digestive enzyme secretion. A large fraction of the cystic fibrosis transmembrane conductance regulator (CFTR), which plays a central role in pancreatic duct HCO(3)(-) secretion, was mislocalized to the cytoplasm of duct cells before treatment. Corticosteroids corrected the localization of CFTR to the apical membrane, accounting for the improved HCO(3)(-) secretion. Steroid treatment resulted in regeneration of acinar cells, accounting for restored digestive enzyme secretion.
Conclusions: Corticosteroids reduce inflammation and restore both digestive enzyme and HCO(3)(-) secretion in patients with AIP by regenerating acinar cells and correcting CFTR localization in pancreatic duct cells. Mislocalization of CFTR may explain aberrant HCO(3)(-) secretion in other forms of pancreatitis.
Copyright 2010 AGA Institute. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
Comment in
-
Pancreas: Autoimmune pancreatitis--mislocalization of CFTR ion channel corrected by corticosteroids.Nat Rev Gastroenterol Hepatol. 2010 Jul;7(7):360. doi: 10.1038/nrgastro.2010.89. Nat Rev Gastroenterol Hepatol. 2010. PMID: 20626076 No abstract available.
Similar articles
-
Restoration of CFTR Activity in Ducts Rescues Acinar Cell Function and Reduces Inflammation in Pancreatic and Salivary Glands of Mice.Gastroenterology. 2017 Oct;153(4):1148-1159. doi: 10.1053/j.gastro.2017.06.011. Epub 2017 Jun 19. Gastroenterology. 2017. PMID: 28634110 Free PMC article.
-
Physiology and pathophysiology of bicarbonate secretion by pancreatic duct epithelium.Nagoya J Med Sci. 2012 Feb;74(1-2):1-18. Nagoya J Med Sci. 2012. PMID: 22515107 Free PMC article. Review.
-
Aquaporin 1 water channel is overexpressed in the plasma membranes of pancreatic ducts in patients with autoimmune pancreatitis.J Med Invest. 2009;56 Suppl:318-21. doi: 10.2152/jmi.56.318. J Med Invest. 2009. PMID: 20224214
-
The Physiology and Pathophysiology of Pancreatic Ductal Secretion: The Background for Clinicians.Pancreas. 2015 Nov;44(8):1211-33. doi: 10.1097/MPA.0000000000000421. Pancreas. 2015. PMID: 26465950 Review.
-
Evaluation of pancreatic endocrine and exocrine function in patients with autoimmune pancreatitis.Pancreas. 2007 Mar;34(2):254-9. doi: 10.1097/01.mpa.0000250127.18908.38. Pancreas. 2007. PMID: 17312466
Cited by
-
Cerulein-induced chronic pancreatitis does not require intra-acinar activation of trypsinogen in mice.Gastroenterology. 2013 May;144(5):1076-1085.e2. doi: 10.1053/j.gastro.2013.01.041. Epub 2013 Jan 24. Gastroenterology. 2013. PMID: 23354015 Free PMC article.
-
The acinar-ductal tango in the pathogenesis of acute pancreatitis.Gut. 2011 Apr;60(4):544-52. doi: 10.1136/gut.2010.218461. Epub 2010 Sep 28. Gut. 2011. PMID: 20876773 Free PMC article. Review.
-
Heavy metals in cigarette smoke strongly inhibit pancreatic ductal function and promote development of chronic pancreatitis.Clin Transl Med. 2024 Jun;14(6):e1733. doi: 10.1002/ctm2.1733. Clin Transl Med. 2024. PMID: 38877637 Free PMC article.
-
Restoration of CFTR Activity in Ducts Rescues Acinar Cell Function and Reduces Inflammation in Pancreatic and Salivary Glands of Mice.Gastroenterology. 2017 Oct;153(4):1148-1159. doi: 10.1053/j.gastro.2017.06.011. Epub 2017 Jun 19. Gastroenterology. 2017. PMID: 28634110 Free PMC article.
-
Commensal Flora, is it an Unwelcomed Companion as a Triggering Factor of Autoimmune Pancreatitis?Front Physiol. 2012 Apr 2;3:77. doi: 10.3389/fphys.2012.00077. eCollection 2012. Front Physiol. 2012. PMID: 22485093 Free PMC article.
References
-
- Hamano H, Kawa S, Horiuchi A, et al. High serum IgG4 concentrations in patients with sclerosing pancreatitis. N Engl J Med. 2001;344:732–738. - PubMed
-
- Kloppel G, Luttges J, Lohr M, et al. Autoimmune pancreatitis: pathological, clinical, and immunological features. Pancreas. 2003;27:14–19. - PubMed
-
- Finkelberg DL, Sahani D, Deshpande V, et al. Autoimmune pancreatitis. N Engl J Med. 2006;355:2670–2676. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
