

Review
doi: 10.1053/j.gastro.2010.01.002.
Epub 2010 Jan 18.
History, molecular mechanisms, and endoscopic treatment of Barrett's esophagus
Affiliations
- PMID: 20080098
- PMCID: PMC2853870
- DOI: 10.1053/j.gastro.2010.01.002
Item in Clipboard
Review
History, molecular mechanisms, and endoscopic treatment of Barrett's esophagus
Gastroenterology.
2010 Mar.
Abstract
This report is an adjunct to the American Gastroenterological Association Institute's medical position statement and technical review on the management of Barrett's esophagus, which will be published in the near future. Those documents will consider a number of broad questions on the diagnosis, clinical features, and management of patients with Barrett's esophagus, and the reader is referred to the technical review for an in-depth discussion of those topics. In this report, we review historical, molecular, and endoscopic therapeutic aspects of Barrett's esophagus that are of interest to clinicians and researchers.
Copyright 2010 AGA Institute. Published by Elsevier Inc. All rights reserved.
Figures
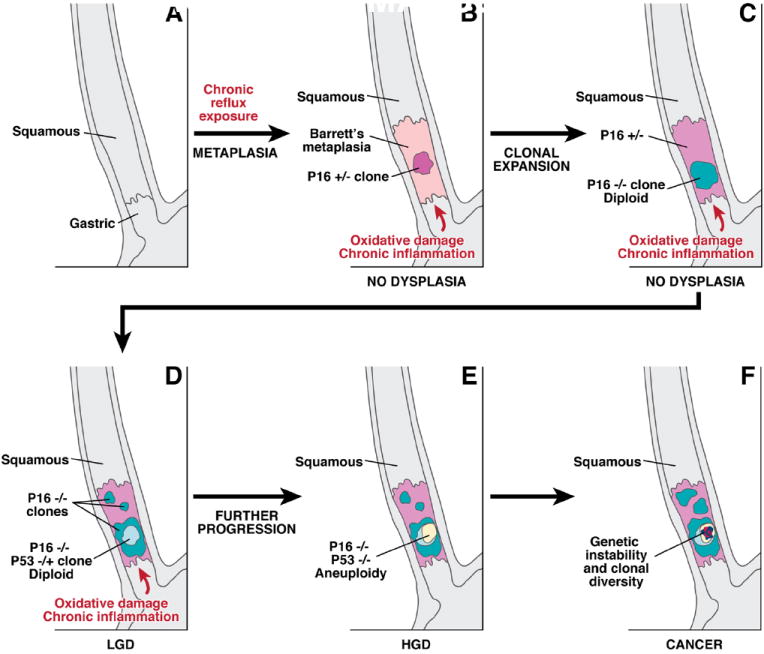
A schematic illustrating the sequential somatic genetic changes in the progression from the squamous esophagus to Barrett’s esophagus to adenocarcinoma. The normal squamous esophagus (A) undergoes a metaplastic transformation with the oxidative damage and chronic inflammation that accompanies chronic gastroesophageal reflux. The initial metaplastic change is followed early on by the loss of one p16 allele (B); this clone may then expand (pink area panel C), followed by loss of the 2nd p16 allele and the formation of some p16 null clones (blue area, C). The subsequent loss of p53 may be associated with morphological changes of low grade dysplasia (LGD), (D). Genetic instability may lead to aneuploidy, which is commonly seen with high grade dysplasia (HGD), (panel E). Numerous clones may develop, and there may be heterogeneity within clones especially as the degree of genetic instability increases and invasive adenocarcinoma develops (F).
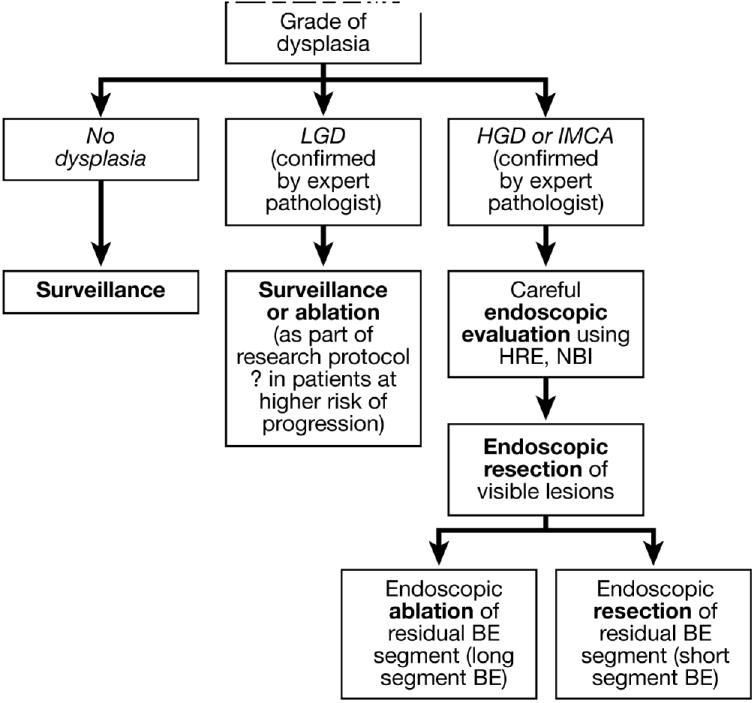
Algorithm for the endoscopic management of dysplasia in Barrett’s esophagus.
Comment in
-
[A dogma changes! Barrett's mucosa without goblet cells?].Z Gastroenterol. 2011 Aug;49(8):1004-6. doi: 10.1055/s-0029-1246099. Epub 2011 Aug 2. Z Gastroenterol. 2011. PMID: 21811953 German. No abstract available.
References
-
- Vakil N, van Zanten SV, Kahrilas P, Dent J, Jones R Global Consensus Group. The Montreal definition and classification of gastroesophageal reflux disease: a global evidence-based consensus. Am J Gastroenterol. 2006;101:1900–20. - PubMed
-
- Barrett NR. Chronic peptic ulcer of the oesophagus and “oesophagitis”. Br J Surg. 1950;38:175–82. - PubMed
-
- Tileston W. Peptic ulcer of the oesophagus. Am J Med Sci. 1906;132:240–65.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
