

Pathways of abdominal tumour spread: the role of the subperitoneal space
- PMID: 20080454
- PMCID: PMC2821589
- DOI: 10.1102/1470-7330.2009.0018
Pathways of abdominal tumour spread: the role of the subperitoneal space
Abstract
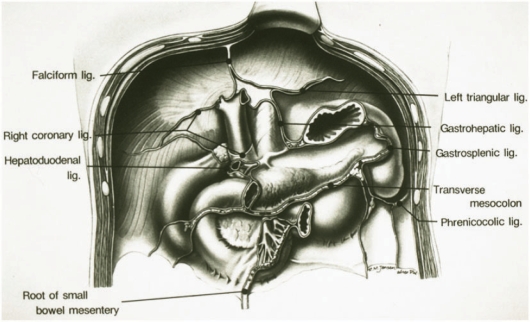
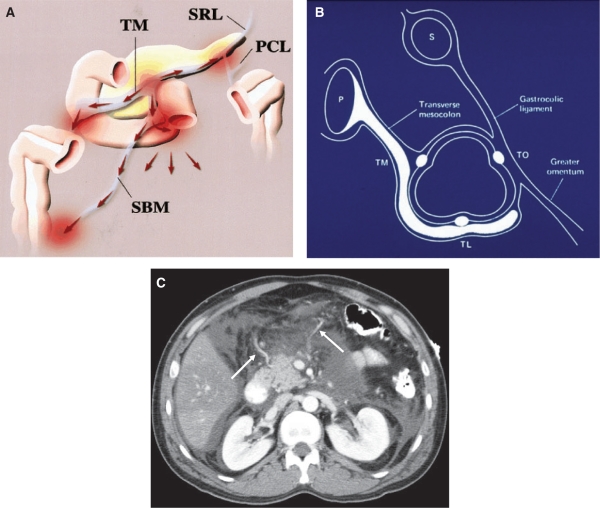
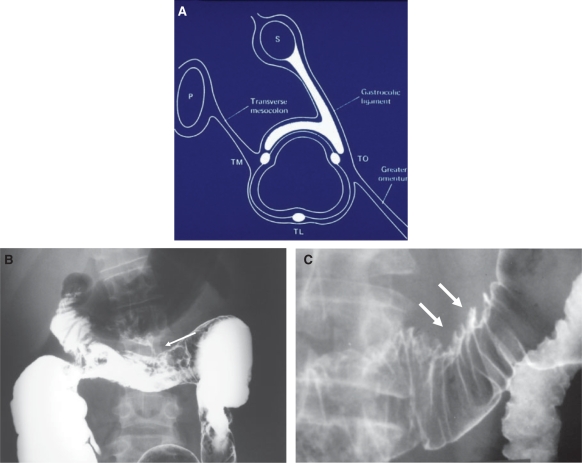
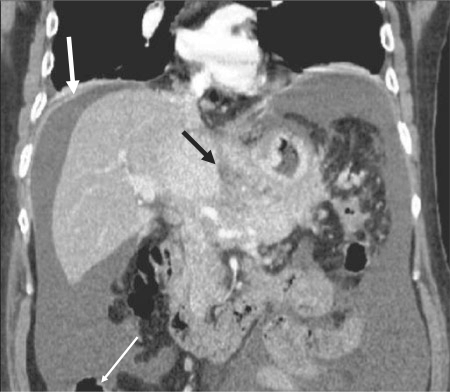
The subperitoneal space is a large, unifying, anatomically continuous potential space that connects the peritoneal cavity with the retroperitoneum. This space is formed by the subserosal areolar tissue that lines the inner surfaces of the peritoneum and the musculature of the abdomen and pelvis. It contains the branches of the vascular, lymphatic, and nervous systems that supply the viscera. The subperitoneal space extends into the peritoneal cavity and is invested between the layers of the mesenteries and ligaments that support and interconnect the abdominal and pelvic organs. As such, it provides one large continuous space in which infectious, neoplastic, inflammatory, and hemorrhagic disease may spread in many directions.
Figures
Similar articles
-
[Subperitoneal space and pathways of abdominal and pelvic tumor spread from the perspective of imaging].Zhonghua Wei Chang Wai Ke Za Zhi. 2020 Aug 25;23(8):810-816. doi: 10.3760/cma.j.cn.441530-20200623-00378. Zhonghua Wei Chang Wai Ke Za Zhi. 2020. PMID: 32810957 Chinese.
-
Subperitoneal extension of disease processes between the chest, abdomen, and the pelvis.Abdom Imaging. 2015 Aug;40(6):1858-70. doi: 10.1007/s00261-014-0297-4. Abdom Imaging. 2015. PMID: 25403702
-
The subperitoneal space and peritoneal cavity: basic concepts.Abdom Imaging. 2015 Oct;40(7):2710-22. doi: 10.1007/s00261-015-0429-5. Abdom Imaging. 2015. PMID: 26006061 Free PMC article.
-
The peritoneum, mesenteries and omenta: normal anatomy and pathological processes.Eur Radiol. 1998;8(6):886-900. doi: 10.1007/s003300050485. Eur Radiol. 1998. PMID: 9683690 Review.
-
Peritoneal and retroperitoneal anatomy and its relevance for cross-sectional imaging.Radiographics. 2012 Mar-Apr;32(2):437-51. doi: 10.1148/rg.322115032. Radiographics. 2012. PMID: 22411941 Review.
Cited by
-
Navigating the labyrinth of peritoneal and extraperitoneal anatomy: abdominal spread made easy with a case based review.Abdom Radiol (NY). 2025 Jan;50(1):379-392. doi: 10.1007/s00261-024-04429-y. Epub 2024 Jun 21. Abdom Radiol (NY). 2025. PMID: 38904709 Free PMC article. Review.
-
Neglected Anatomical Areas in Ovarian Cancer: Significance for Optimal Debulking Surgery.Cancers (Basel). 2024 Jan 9;16(2):285. doi: 10.3390/cancers16020285. Cancers (Basel). 2024. PMID: 38254777 Free PMC article. Review.
References
-
- Borley NR. In: Gray's anatomy. 40th. Philadelphia: WB Saunders; 2009. Peritoneum and peritoneal cavity; pp. 1347–1501.
-
- Oliphant M, Berne AS, Meyers MA. Subperitoneal spread of intra-abdominal disease. In: Meyers MA, editor. Computed tomography of the gastrointestinal tract. New York: Springer-Verlag; 1986. pp. 95–138.
-
- Oliphant M, Berne AS. Computed tomography of the subperitoneal space: demonstration of direct spread of intraabdominal disease. J Comput Assist Tomogr. 1982;6:1127–37. - PubMed
-
- Meyers MA, Oliphant M, Berne AS, et al. The peritoneal ligaments and mesenteries: pathways of intraabdominal spread of disease. Radiology. 1987;163:593–604. - PubMed
-
- Meyers MA. Intraperitoneal spread of infections. In: Meyers MA, editor. Dynamic radiology of the abdomen: normal and pathologic anatomy. 4th. New York: Springer-Verlag; 1993. pp. 55–114.
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials