

Optimizing infectious disease interventions during an emerging epidemic
- PMID: 20080777
- PMCID: PMC2818907
- DOI: 10.1073/pnas.0908491107
Optimizing infectious disease interventions during an emerging epidemic
Abstract
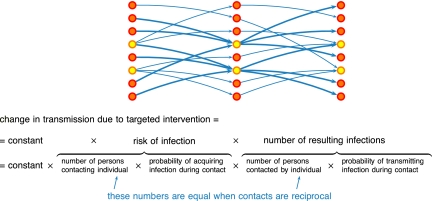
The emergence and global impact of the novel influenza A(H1N1)v highlights the continuous threat to public health posed by a steady stream of new and unexpected infectious disease outbreaks in animals and humans. Once an emerging epidemic is detected, public health authorities will attempt to mitigate the epidemic by, among other measures, reducing further spread as much as possible. Scarce and/or costly control measures such as vaccines, anti-infective drugs, and social distancing must be allocated while epidemiological characteristics of the disease remain uncertain. Here we present first principles for allocating scarce resources with limited data. We show that under a broad class of assumptions, the simple rule of targeting intervention measures at the group with the highest risk of infection per individual will achieve the largest reduction in the transmission potential of a novel infection. For vaccination of susceptible persons, the appropriate risk measure is force of infection; for social distancing, the appropriate risk measure is incidence of infection. Unlike existing methods that rely on detailed knowledge of group-specific transmission rates, the method described here can be implemented using only data that are readily available during an epidemic, and allows ready adaptation as the epidemic progresses. The need to observe risk of infection helps to focus the ongoing planning and design of new infectious disease surveillance programs; from the presented first principles for allocating scarce resources, we can adjust the prioritization of groups for intervention when new observations on an emerging epidemic become available.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Tildesley MJ, et al. Optimal reactive vaccination strategies for a foot-and-mouth outbreak in the UK. Nature. 2006;440:83–86. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
