

Epidermal injury and infection during poxvirus immunization is crucial for the generation of highly protective T cell-mediated immunity
- PMID: 20081864
- PMCID: PMC3070948
- DOI: 10.1038/nm.2078
Epidermal injury and infection during poxvirus immunization is crucial for the generation of highly protective T cell-mediated immunity
Abstract
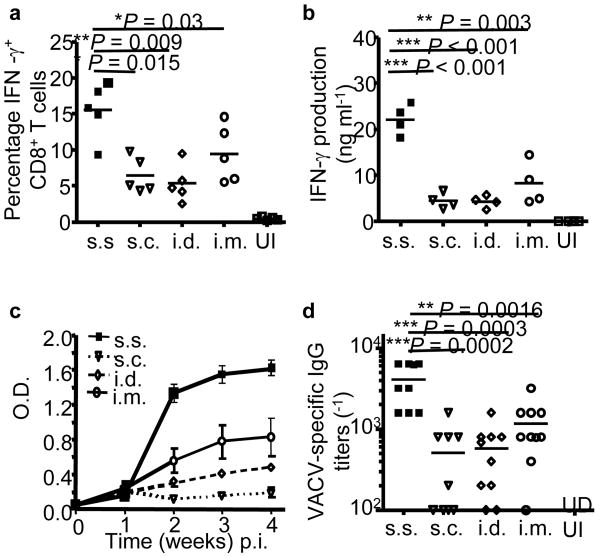
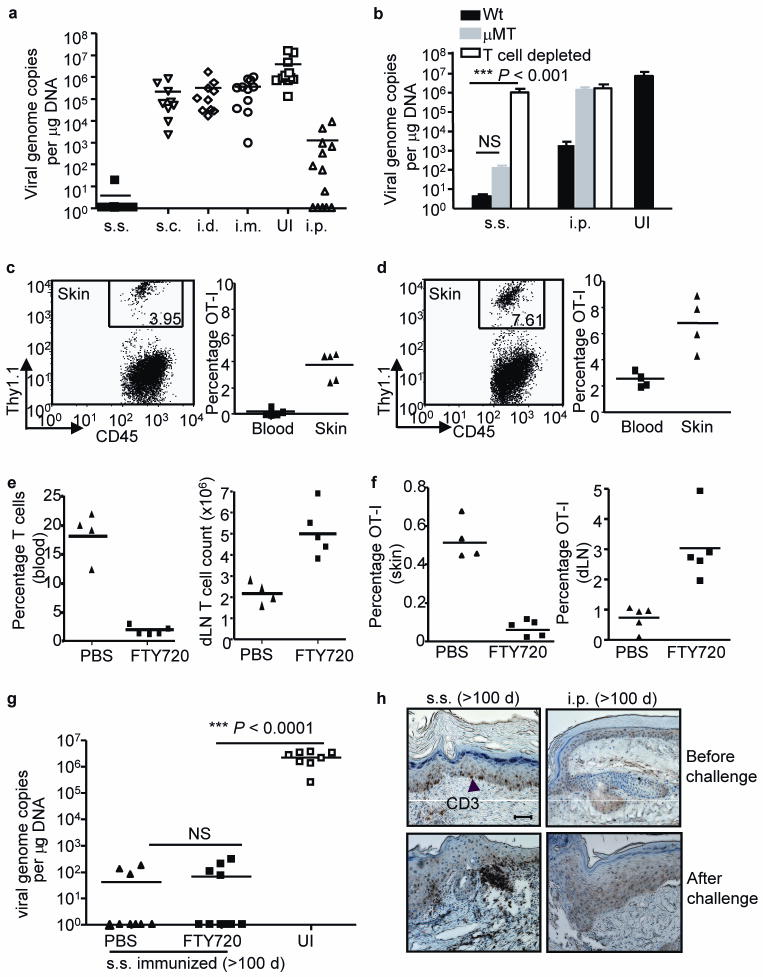
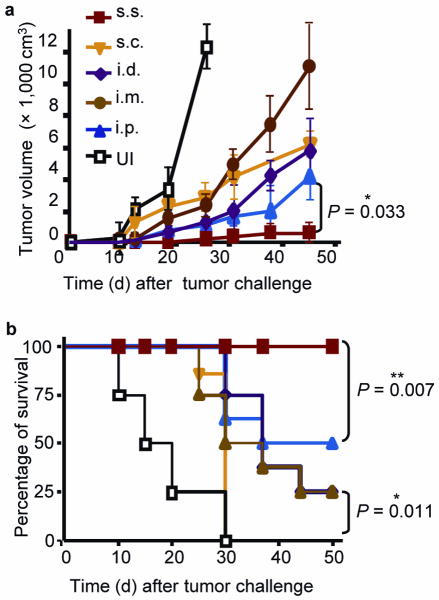
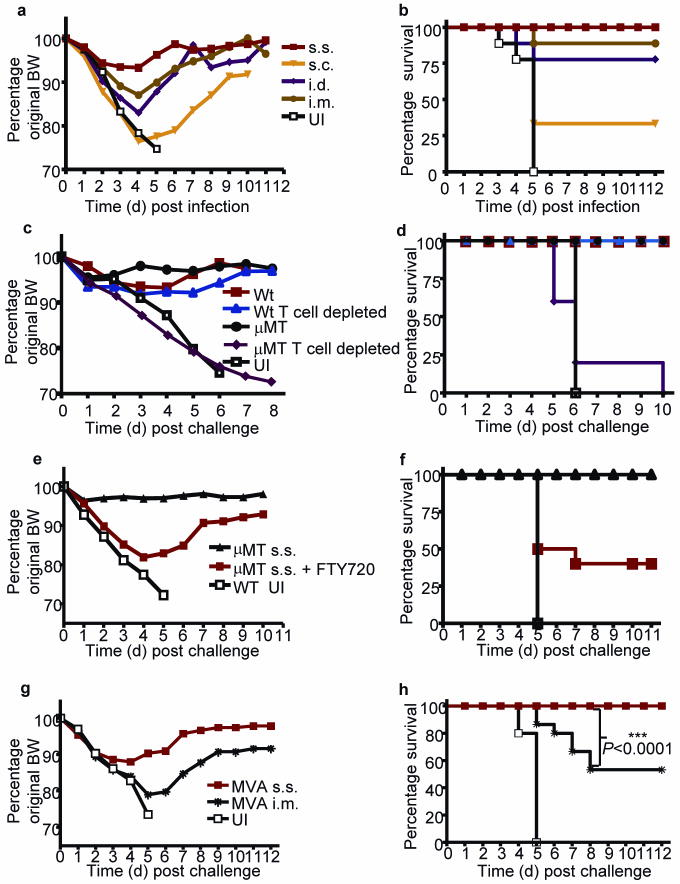
Variola major (smallpox) infection claimed hundreds of millions lives before it was eradicated by a simple vaccination strategy: epicutaneous application of the related orthopoxvirus vaccinia virus (VACV) to superficially injured skin (skin scarification, s.s.). However, the remarkable success of this strategy was attributed to the immunogenicity of VACV rather than to the unique mode of vaccine delivery. We now show that VACV immunization via s.s., but not conventional injection routes, is essential for the generation of superior T cell-mediated immune responses that provide complete protection against subsequent challenges, independent of neutralizing antibodies. Skin-resident effector memory T cells (T(EM) cells) provide complete protection against cutaneous challenge, whereas protection against lethal respiratory challenge requires both respiratory mucosal T(EM) cells and central memory T cells (T(CM) cells). Vaccination with recombinant VACV (rVACV) expressing a tumor antigen was protective against tumor challenge only if delivered via the s.s. route; it was ineffective if delivered by hypodermic injection. The clinically safer nonreplicative modified vaccinia Ankara virus (MVA) also generated far superior protective immunity when delivered via the s.s. route compared to intramuscular (i.m.) injection as used in MVA clinical trials. Thus, delivery of rVACV-based vaccines, including MVA vaccines, through physically disrupted epidermis has clear-cut advantages over conventional vaccination via hypodermic injection.
Figures
References
-
- Stewart AJ, Devlin PM. The history of the smallpox vaccine. J Infect. 2006;52:329–334. - PubMed
-
- Hammarlund E, et al. Duration of antiviral immunity after smallpox vaccination. Nat Med. 2003;9:1131–1137. - PubMed
-
- Liu L, Fuhlbrigge RC, Karibian K, Tian T, Kupper TS. Dynamic programming of CD8+ T cell trafficking after live viral immunization. Immunity. 2006;25:511–520. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
