

Effect of obesity and low back pain on spinal mobility: a cross sectional study in women
- PMID: 20082692
- PMCID: PMC2821381
- DOI: 10.1186/1743-0003-7-3
Effect of obesity and low back pain on spinal mobility: a cross sectional study in women
Abstract
Background: obesity is nowadays a pandemic condition. Obese subjects are commonly characterized by musculoskeletal disorders and particularly by non-specific chronic low back pain (cLBP). However, the relationship between obesity and cLBP remains to date unsupported by an objective measurement of the mechanical behaviour of the spine and its morphology in obese subjects. Such analysis may provide a deeper understanding of the relationships between function and the onset of clinical symptoms.
Purpose: to objectively assess the posture and function of the spine during standing, flexion and lateral bending in obese subjects with and without cLBP and to investigate the role of obesity in cLBP.
Study design: Cross-sectional study
Patient sample: thirteen obese subjects, thirteen obese subjects with cLBP, and eleven healthy subjects were enrolled in this study.
Outcome measures: we evaluated the outcome in terms of angles at the initial standing position (START) and at maximum forward flexion (MAX). The range of motion (ROM) between START and MAX was also computed.
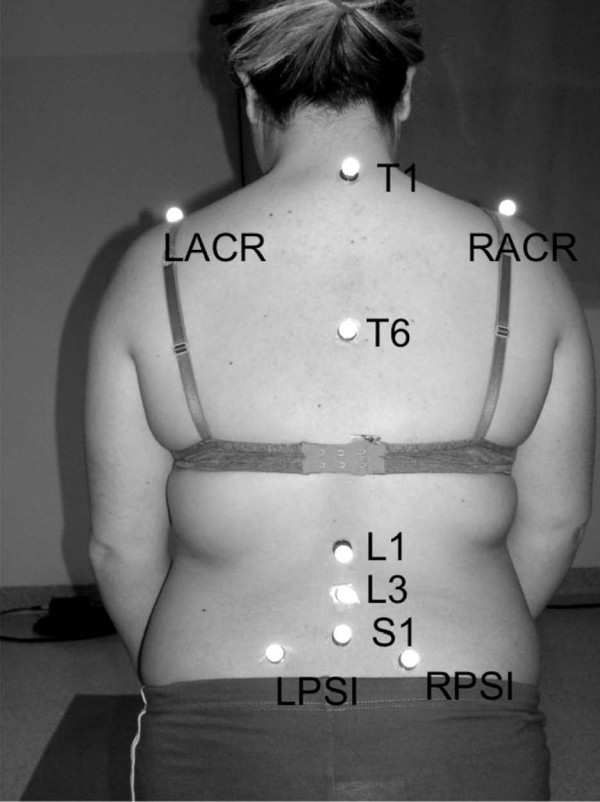
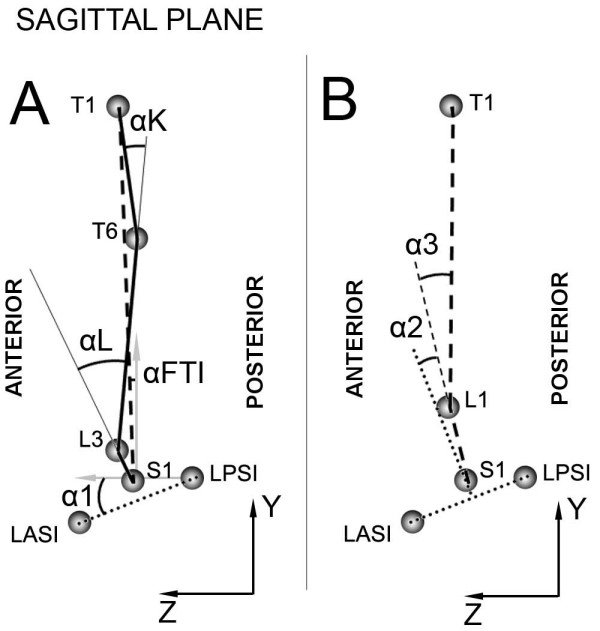
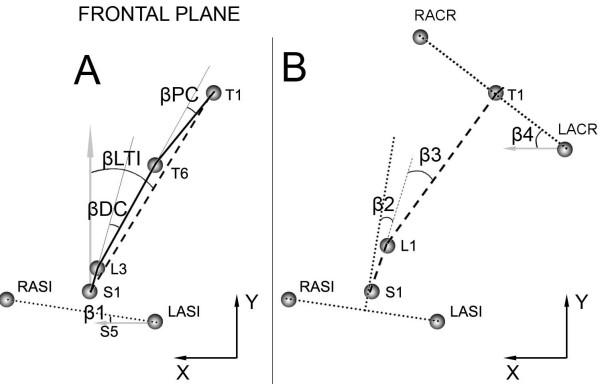
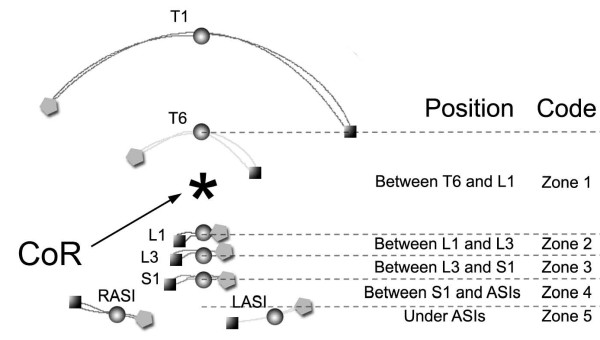
Methods: we studied forward flexion and lateral bending of the spine using an optoelectronic system and passive retroreflective markers applied on the trunk. A biomechanical model was developed in order to analyse kinematics and define angles of clinical interest.
Results: obesity was characterized by a generally reduced ROM of the spine, due to a reduced mobility at both pelvic and thoracic level; a static postural adaptation with an increased anterior pelvic tilt. Obesity with cLBP is associated with an increased lumbar lordosis.In lateral bending, obesity with cLBP is associated with a reduced ROM of the lumbar and thoracic spine, whereas obesity on its own appears to affect only the thoracic curve.
Conclusions: obese individuals with cLBP showed higher degree of spinal impairment when compared to those without cLBP. The observed obesity-related thoracic stiffness may characterize this sub-group of patients, even if prospective studies should be carried out to verify this hypothesis.
Figures
Similar articles
-
Lumbar Spine Alignment in Six Common Postures: An ROM Analysis With Implications for Deformity Correction.Spine (Phila Pa 1976). 2017 Oct 1;42(19):1447-1455. doi: 10.1097/BRS.0000000000002131. Spine (Phila Pa 1976). 2017. PMID: 28240654
-
Relative mobility of the pelvis and spine during trunk axial rotation in chronic low back pain patients: A case-control study.PLoS One. 2017 Oct 17;12(10):e0186369. doi: 10.1371/journal.pone.0186369. eCollection 2017. PLoS One. 2017. PMID: 29040298 Free PMC article.
-
Differences in standing and forward bending in women with chronic low back or pelvic girdle pain: indications for physical compensation strategies.Spine (Phila Pa 1976). 2008 May 15;33(11):E334-41. doi: 10.1097/BRS.0b013e318170fcf6. Spine (Phila Pa 1976). 2008. PMID: 18469680
-
Effects of cycling on the morphology and spinal posture in professional and recreational cyclists: a systematic review.Sports Biomech. 2023 Apr;22(4):567-596. doi: 10.1080/14763141.2022.2058990. Epub 2022 Apr 19. Sports Biomech. 2023. PMID: 35440291
-
Spinopelvic Compensatory Mechanisms for Reduced Hip Motion (ROM) in the Setting of Hip Osteoarthritis.Spine Deform. 2019 Nov;7(6):923-928. doi: 10.1016/j.jspd.2019.03.007. Spine Deform. 2019. PMID: 31732003 Review.
Cited by
-
Best Evidence Rehabilitation for Chronic Pain Part 3: Low Back Pain.J Clin Med. 2019 Jul 19;8(7):1063. doi: 10.3390/jcm8071063. J Clin Med. 2019. PMID: 31331087 Free PMC article.
-
Changes in Back Pain Scores after Bariatric Surgery in Obese Patients: A Systematic Review and Meta-Analysis.J Clin Med. 2021 Apr 1;10(7):1443. doi: 10.3390/jcm10071443. J Clin Med. 2021. PMID: 33916220 Free PMC article. Review.
-
Effects of triple-treatment trunk stretching on physical fitness and curvature of the spine.Heliyon. 2018 Dec 1;4(12):e00985. doi: 10.1016/j.heliyon.2018.e00985. eCollection 2018 Dec. Heliyon. 2018. PMID: 30534617 Free PMC article.
-
Validation and Estimation of Obesity-Induced Intervertebral Disc Degeneration through Subject-Specific Finite Element Modelling of Functional Spinal Units.Bioengineering (Basel). 2024 Mar 31;11(4):344. doi: 10.3390/bioengineering11040344. Bioengineering (Basel). 2024. PMID: 38671766 Free PMC article.
-
A framework of biomarkers for skeletal aging: a consensus statement by the Aging Biomarker Consortium.Life Med. 2023 Nov 22;2(6):lnad045. doi: 10.1093/lifemedi/lnad045. eCollection 2023 Dec. Life Med. 2023. PMID: 39872060 Free PMC article.
References
-
- Hinton R, Moody RL, Davis AW, Thomas SF. Osteoarthritis: diagnosis and therapeutic considerations. Am Fam Physician. 2002;65:841–848. - PubMed
