

Cost-effectiveness of collaborative care for the treatment of major depressive disorder in primary care. A systematic review
- PMID: 20082727
- PMCID: PMC2826303
- DOI: 10.1186/1472-6963-10-19
Cost-effectiveness of collaborative care for the treatment of major depressive disorder in primary care. A systematic review
Abstract
Background: The effectiveness of collaborative care for patients with major depressive disorder in primary care has been established. Assessing its cost-effectiveness is important for deciding on implementation. This review therefore evaluates the cost-effectiveness of collaborative care for major depressive disorder in primary care.
Methods: A systematic search on economic evaluations of collaborative care was conducted in Pubmed and PsychInfo. Quality of the studies was measured with the Cochrane checklist and the CHEC-list for economic evaluations. Cost-effectiveness and costs per depression-free days were reported.
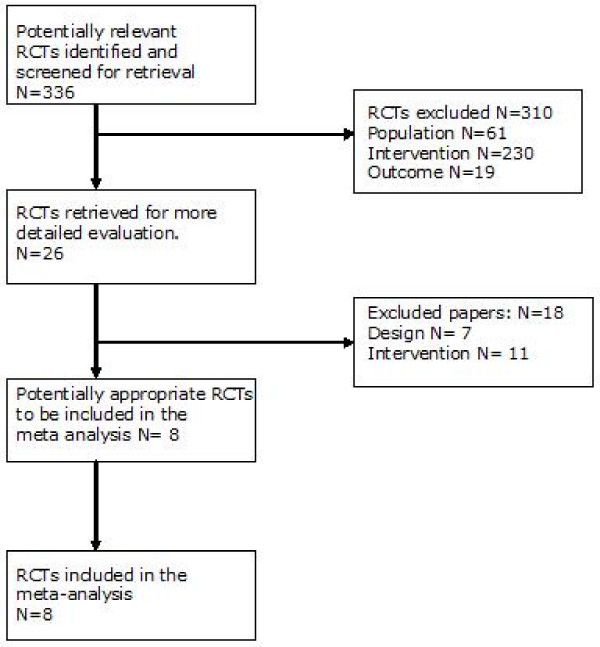
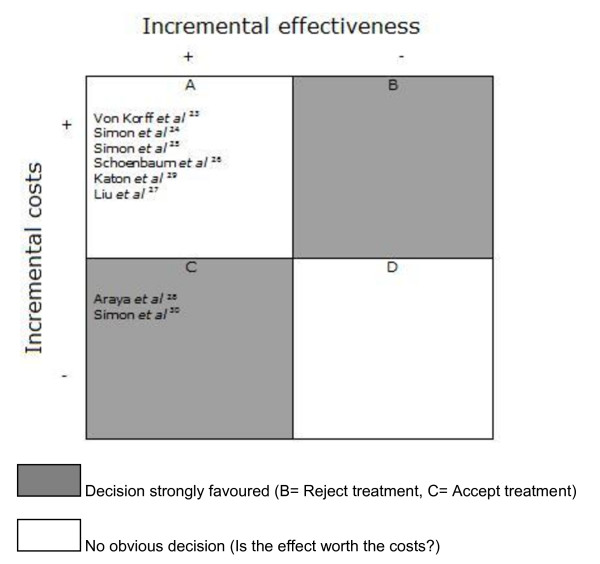
Results: 8 studies were found, involving 4868 patients. The quality of the cost effectiveness studies, according to the CHEC-list, could be improved. Generally, the studies did not include all relevant costs and did not perform sensitivity analysis. Only 4 out of 8 studies reported cost per QALY, 6 out of 8 reported costs per depression-free days. The highest costs per QALY reported were $49,500, the highest costs per depression-free day were $24.
Conclusions: Although studies did not fulfil all criteria of the CHEC-list, collaborative care is a promising intervention and it may be cost-effective. However, to conclude on the cost-effectiveness, depression research should follow economic guidelines to improve the quality of the economic evaluations.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
