

Cancellations of (helicopter-transported) mobile medical team dispatches in the Netherlands
- PMID: 20084394
- PMCID: PMC2908760
- DOI: 10.1007/s00423-009-0576-7
Cancellations of (helicopter-transported) mobile medical team dispatches in the Netherlands
Abstract
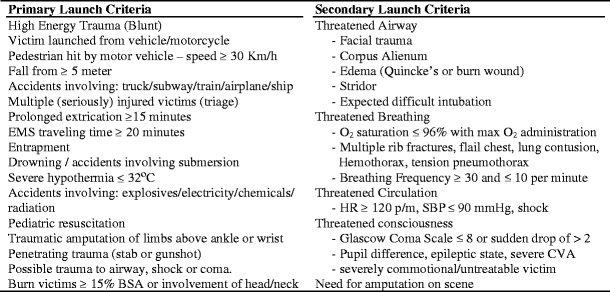
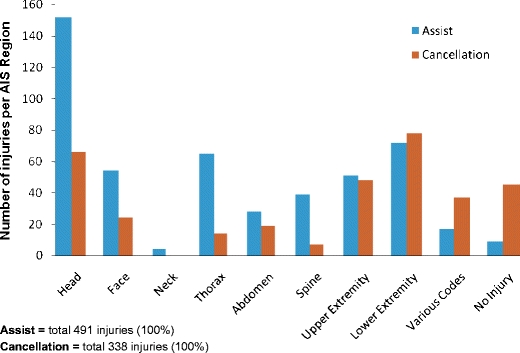
Background: The trauma centre of the Trauma Center Region North-West Netherlands (TRNWN) has consensus criteria for Mobile Medical Team (MMT) scene dispatch. The MMT can be dispatched by the EMS-dispatch centre or by the on-scene ambulance crew and is transported by helicopter or ground transport. Although much attention has been paid to improve the dispatch criteria, the MMT is often cancelled after being dispatched. The aim of this study was to assess the cancellation rate and the noncompliant dispatches of our MMT and to identify factors associated with this form of primary overtriage.
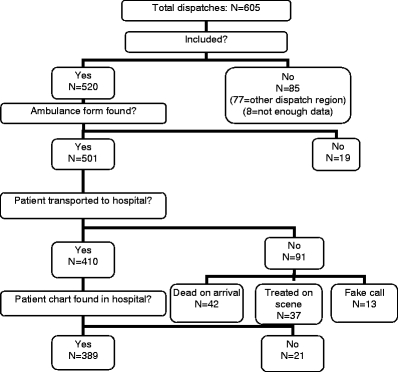
Methods: By retrospective analysis of all MMT dispatches in the period from 1 July 2006 till 31 December 2006 using chart review, we conducted a consecutive case review of 605 dispatches. Four hundred and sixty seven of these were included for our study, collecting data related to prehospital triage, patient's condition on-scene and hospital course.
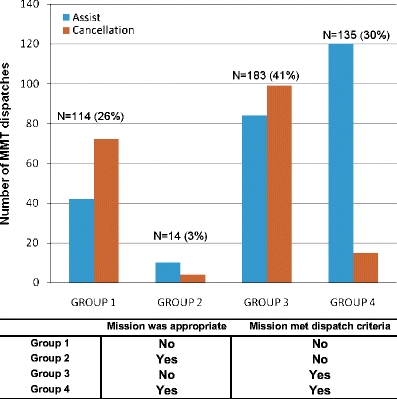
Results: Average age was 35.9 years; the majority of the patients were male (65.3%). Four hundred and thirty patients were victims of trauma, sustaining injuries in most cases from blunt trauma (89.3%). After being dispatched, the MMT was cancelled 203 times (43.5%). Statistically significant differences between assists and cancellations were found for overall mortality, mean RTS, GCS and ISS, mean hospitalization, length and amount of ICU admissions (p < 0.001). All dispatches were evaluated by using the MMT-dispatch criteria and mission appropriateness criteria. Almost 26% of all dispatches were neither appropriate, nor met the dispatch criteria. Fourteen missions were appropriate, but did not meet the dispatch criteria. The remaining 318 dispatches had met the dispatch criteria, of which 135 (30.3%) were also appropriate. The calculated additional costs of the cancelled dispatches summed up to a total of 34,448 euro, amounting to 2.2% of the total MMT costs during the study period.
Conclusion: In our trauma system, the MMT dispatches are involved with high rates of overtriage. After being dispatched, the MMT is cancelled in almost 50% of all cases. We found an undertriage rate of 4%, which we think is acceptable. All cancellations were justified. The additional costs of the cancelled missions were within an acceptable range. According to this study, it seems to be possible to reduce the overtriage rate of the MMT dispatches, without increasing the undertriage rate to non-acceptable levels.
Figures
Comment in
-
Human errors in (inhuman?) triage.Langenbecks Arch Surg. 2010 Nov;395(8):1175-6; author reply 1177-8. doi: 10.1007/s00423-010-0610-9. Epub 2010 Jun 30. Langenbecks Arch Surg. 2010. PMID: 20589394 No abstract available.
Similar articles
-
Characteristics of helicopter emergency medical services (HEMS) dispatch cancellations during a six-year period in a Dutch HEMS region.BMC Emerg Med. 2021 Apr 16;21(1):50. doi: 10.1186/s12873-021-00439-x. BMC Emerg Med. 2021. PMID: 33863280 Free PMC article.
-
Criteria for cancelling helicopter emergency medical services (HEMS) dispatches.Emerg Med J. 2012 Jul;29(7):582-6. doi: 10.1136/emj.2011.112896. Epub 2011 Jul 23. Emerg Med J. 2012. PMID: 21785150
-
Is a maximum Revised Trauma Score a safe triage tool for Helicopter Emergency Medical Services cancellations?Eur J Emerg Med. 2011 Aug;18(4):197-201. doi: 10.1097/MEJ.0b013e328344912e. Eur J Emerg Med. 2011. PMID: 21326101
-
Trauma-related dispatch criteria for Helicopter Emergency Medical Services in Europe.Injury. 2011 May;42(5):525-33. doi: 10.1016/j.injury.2010.03.015. Epub 2010 Apr 9. Injury. 2011. PMID: 20381803 Review.
-
[Prehospital triage in trauma patients; ambulance care and deployment of a mobile medical team].Ned Tijdschr Geneeskd. 2017;161:D1579. Ned Tijdschr Geneeskd. 2017. PMID: 28513414 Review. Dutch.
Cited by
-
Characteristics of helicopter emergency medical services (HEMS) dispatch cancellations during a six-year period in a Dutch HEMS region.BMC Emerg Med. 2021 Apr 16;21(1):50. doi: 10.1186/s12873-021-00439-x. BMC Emerg Med. 2021. PMID: 33863280 Free PMC article.
-
Helicopter-based emergency medical services for a sparsely populated region: A study of 42,500 dispatches.Acta Anaesthesiol Scand. 2016 May;60(5):659-67. doi: 10.1111/aas.12673. Epub 2015 Dec 21. Acta Anaesthesiol Scand. 2016. PMID: 26810562 Free PMC article.
-
A novel method of non-clinical dispatch is associated with a higher rate of critical Helicopter Emergency Medical Service intervention.Scand J Trauma Resusc Emerg Med. 2018 Sep 25;26(1):84. doi: 10.1186/s13049-018-0551-9. Scand J Trauma Resusc Emerg Med. 2018. PMID: 30253795 Free PMC article.
-
FAST and undertriage.Langenbecks Arch Surg. 2010 Jun;395(5):595-6. doi: 10.1007/s00423-010-0624-3. Epub 2010 May 29. Langenbecks Arch Surg. 2010. PMID: 20512351 No abstract available.
-
Characteristics of patients treated by the Danish Helicopter Emergency Medical Service from 2014-2018: a nationwide population-based study.Scand J Trauma Resusc Emerg Med. 2019 Nov 7;27(1):102. doi: 10.1186/s13049-019-0672-9. Scand J Trauma Resusc Emerg Med. 2019. PMID: 31699120 Free PMC article.
References
-
- Surgeons Committee on Trauma—American College of Surgeons . Resources for optimal care of the injured patient. Chicago: American College of Surgeons; 1998.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
