

Inadequacy of plasma acyclovir levels at delivery in patients with genital herpes receiving oral acyclovir suppressive therapy in late pregnancy
- PMID: 20085679
- PMCID: PMC2809929
- DOI: 10.1016/s1701-2163(16)34374-2
Inadequacy of plasma acyclovir levels at delivery in patients with genital herpes receiving oral acyclovir suppressive therapy in late pregnancy
Abstract
Objective: Acyclovir therapy in late pregnancy among women with recurrent genital herpes is effective in decreasing genital lesion frequency and subclinical viral shedding rates at delivery, thereby decreasing the need for Caesarean section. Despite good adherence and increased dosing schedules, breakthrough lesions and viral shedding are still observed in some women at or near delivery. Anecdotal evidence suggests that low levels of herpes simplex virus replication at delivery may result in transmission to the neonate. Therefore, defining optimal acyclovir dosing during labour and delivery is warranted. Our objectives were to determine actual maternal and fetal acyclovir levels at delivery, and explore associations between acyclovir levels, duration of labour, and time since last acyclovir dose.
Methods: Twenty-seven patients were prescribed oral acyclovir 400 mg three times daily from 36 weeks' gestation. Cord blood (venous and arterial) and maternal venous blood samples were collected at delivery, and acyclovir levels measured using capillary electrophoresis. Correlations between duration of labour, and time since last acyclovir dose with acyclovir blood levels were calculated.
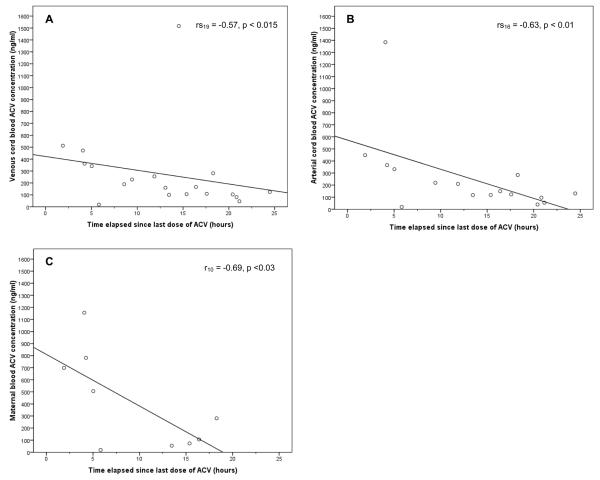
Results: Acyclovir levels were below the published mean steady-state trough value (180 ng/mL) in 52% of venous cord samples, 55% of arterial cord samples, and 36% of maternal samples. There was a significant inverse correlation between the time since last dose and venous cord levels (rs19 = -0.57, P < 0.015), arterial cord levels (rs16 = -0.63, P < 0.01), and maternal acyclovir levels (r10 = -0.69, P < 0.03).
Conclusion: Oral dosing of acyclovir in women in late pregnancy may result in insufficient levels at delivery to prevent viral shedding. Alternative approaches that incorporate acyclovir dosing through labour, either through oral or intravenous administration, should be evaluated to assess effects on viral shedding.
Figures
Similar articles
-
Oral acyclovir and recurrent genital herpes during late pregnancy.Obstet Gynecol. 1993 Jul;82(1):102-4. Obstet Gynecol. 1993. PMID: 8390630
-
Acyclovir prophylaxis in late pregnancy to prevent neonatal herpes: a cost-effectiveness analysis.Obstet Gynecol. 1996 Oct;88(4 Pt 1):603-10. doi: 10.1016/0029-7844(96)00261-x. Obstet Gynecol. 1996. PMID: 8841227
-
Acyclovir suppression to prevent recurrent genital herpes at delivery.Infect Dis Obstet Gynecol. 2002;10(2):71-7. doi: 10.1155/S1064744902000054. Infect Dis Obstet Gynecol. 2002. PMID: 12530483 Free PMC article. Clinical Trial.
-
Prevention of perinatal herpes: prophylactic antiviral therapy?Clin Obstet Gynecol. 1999 Mar;42(1):134-48; quiz 174-5. doi: 10.1097/00003081-199903000-00018. Clin Obstet Gynecol. 1999. PMID: 10073307 Review.
-
Vertical transmission of genital herpes: prevention and treatment options.Drugs. 2009;69(4):421-34. doi: 10.2165/00003495-200969040-00003. Drugs. 2009. PMID: 19323586 Review.
Cited by
-
Mechanistic Modeling of Placental Drug Transfer in Humans: How Do Differences in Maternal/Fetal Fraction of Unbound Drug and Placental Influx/Efflux Transfer Rates Affect Fetal Pharmacokinetics?Front Pediatr. 2021 Oct 18;9:723006. doi: 10.3389/fped.2021.723006. eCollection 2021. Front Pediatr. 2021. PMID: 34733804 Free PMC article.
-
Prediction of Maternal and Fetal Acyclovir, Emtricitabine, Lamivudine, and Metformin Concentrations during Pregnancy Using a Physiologically Based Pharmacokinetic Modeling Approach.Clin Pharmacokinet. 2022 May;61(5):725-748. doi: 10.1007/s40262-021-01103-0. Epub 2022 Jan 24. Clin Pharmacokinet. 2022. PMID: 35067869
-
Physiologically Based Pharmacokinetic Models to Predict Maternal Pharmacokinetics and Fetal Exposure to Emtricitabine and Acyclovir.J Clin Pharmacol. 2020 Feb;60(2):240-255. doi: 10.1002/jcph.1515. Epub 2019 Sep 6. J Clin Pharmacol. 2020. PMID: 31489678 Free PMC article.
References
-
- Fonnest G, Fonnest ID, Weber T. Neonatal herpes in Denmark 1977-1991. Acta Obstet Gynecol Scand. 1997;76(4):355–8. - PubMed
-
- Poeran J, Wildschut H, Gaytant M, Galama J, Steegers E, van der Meijden W. The incidence of neonatal herpes in The Netherlands. J Clin Virol. 2008;42(4):321–5. - PubMed
-
- Tookey P, Peckham CS. Neonatal herpes simplex virus infection in the British Isles. Paed Perinatal Epidemiol. 1996;10(4):432–42. - PubMed
-
- Kropp RY, Wong T, Cormier L, Ringrose A, Burton S, Embree JE, Steben M. Neonatal herpes simplex virus infections in Canada: Results of a 3-year national prospective study. Pediatrics. 2006;117(6):1955–62. - PubMed
-
- Garland SM. Neonatal Herpes-Simplex - Royal-Womens-Hospital 10-Year Experience with Management Guidelines for Herpes in Pregnancy. Aust NZ J Obstet Gynaecol. 1992;32(4):331–4. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
