

Assessing the cost effectiveness of using prognostic biomarkers with decision models: case study in prioritising patients waiting for coronary artery surgery
- PMID: 20085988
- PMCID: PMC2808469
- DOI: 10.1136/bmj.b5606
Assessing the cost effectiveness of using prognostic biomarkers with decision models: case study in prioritising patients waiting for coronary artery surgery
Abstract
Objective: To determine the effectiveness and cost effectiveness of using information from circulating biomarkers to inform the prioritisation process of patients with stable angina awaiting coronary artery bypass graft surgery.
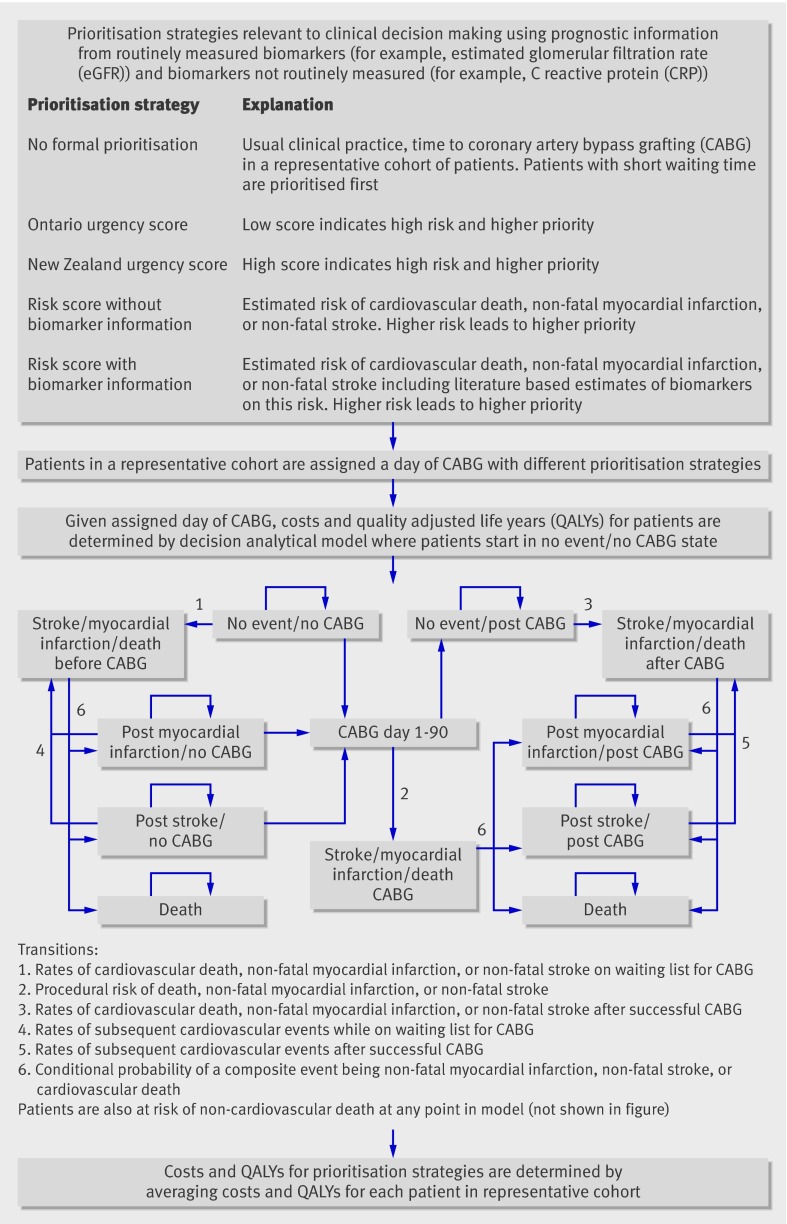
Design: Decision analytical model comparing four prioritisation strategies without biomarkers (no formal prioritisation, two urgency scores, and a risk score) and three strategies based on a risk score using biomarkers: a routinely assessed biomarker (estimated glomerular filtration rate), a novel biomarker (C reactive protein), or both. The order in which to perform coronary artery bypass grafting in a cohort of patients was determined by each prioritisation strategy, and mean lifetime costs and quality adjusted life years (QALYs) were compared.
Data sources: Swedish Coronary Angiography and Angioplasty Registry (9935 patients with stable angina awaiting coronary artery bypass grafting and then followed up for cardiovascular events after the procedure for 3.8 years), and meta-analyses of prognostic effects (relative risks) of biomarkers.
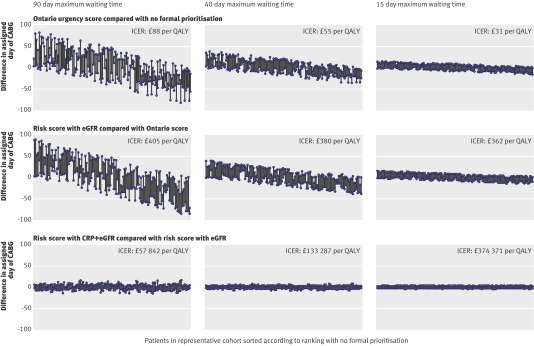
Results: The observed risk of cardiovascular events while on the waiting list for coronary artery bypass grafting was 3 per 10,000 patients per day within the first 90 days (184 events in 9935 patients). Using a cost effectiveness threshold of pound20,000- pound30,000 (euro22,000-euro33,000; $32,000-$48,000) per additional QALY, a prioritisation strategy using a risk score with estimated glomerular filtration rate was the most cost effective strategy (cost per additional QALY was < pound410 compared with the Ontario urgency score). The impact on population health of implementing this strategy was 800 QALYs per 100,000 patients at an additional cost of pound 245,000 to the National Health Service. The prioritisation strategy using a risk score with C reactive protein was associated with lower QALYs and higher costs compared with a risk score using estimated glomerular filtration rate.
Conclusion: Evaluating the cost effectiveness of prognostic biomarkers is important even when effects at an individual level are small. Formal prioritisation of patients awaiting coronary artery bypass grafting using a routinely assessed biomarker (estimated glomerular filtration rate) along with simple, routinely collected clinical information was cost effective. Prioritisation strategies based on the prognostic information conferred by C reactive protein, which is not currently measured in this context, or a combination of C reactive protein and estimated glomerular filtration rate, is unlikely to be cost effective. The widespread practice of using only implicit or informal means of clinically ordering the waiting list may be harmful and should be replaced with formal prioritisation approaches.
Conflict of interest statement
Competing interests: All authors have completed the unified competing interest form at
Figures
Comment in
-
Using biomarkers to prioritise patients with stable angina pectoris for bypass surgery.BMJ. 2010 Jan 20;340:b5414. doi: 10.1136/bmj.b5414. BMJ. 2010. PMID: 20089597 No abstract available.
References
-
- Moons KG, Royston P, Vergouwe Y, Grobbee DE, Altman DG. Prognosis and prognostic research: what, why, and how? BMJ 2009;338:b375. - PubMed
-
- Hemingway H. Prognosis research: why is Dr Lydgate still waiting? J Clin Epidemiol 2006;59:1229-38. - PubMed
-
- Hemingway H, Riley RD, Altman DG. Ten steps to improving prognosis research. BMJ 2009;339:b4184. - PubMed
-
- Vasan RS. Biomarkers of cardiovascular disease: molecular basis and practical considerations. Circulation 2006;113:2335-62. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials