

Home based versus centre based cardiac rehabilitation: Cochrane systematic review and meta-analysis
- PMID: 20085991
- PMCID: PMC2808470
- DOI: 10.1136/bmj.b5631
Home based versus centre based cardiac rehabilitation: Cochrane systematic review and meta-analysis
Erratum in
- BMJ. 2010;340:c1133
Abstract
Objective: To compare the effect of home based and supervised centre based cardiac rehabilitation on mortality and morbidity, health related quality of life, and modifiable cardiac risk factors in patients with coronary heart disease.
Design: Systematic review.
Data sources: Cochrane Central Register of Controlled Trials (CENTRAL) in the Cochrane Library, Medline, Embase, CINAHL, and PsycINFO, without language restriction, searched from 2001 to January 2008.
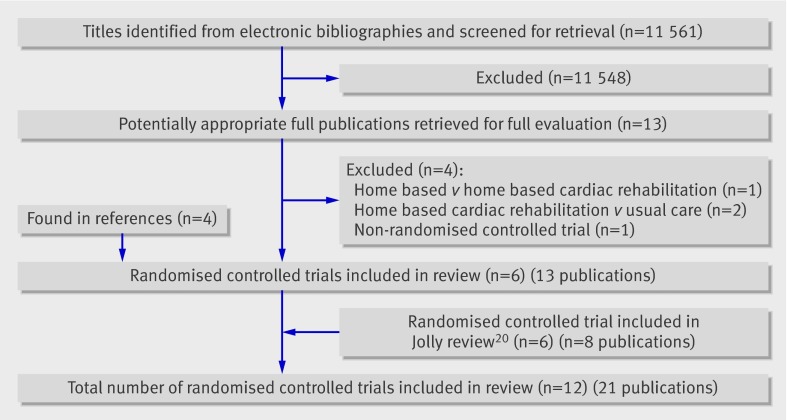
Review methods: Reference lists checked and advice sought from authors. Included randomised controlled trials that compared centre based cardiac rehabilitation with home based programmes in adults with acute myocardial infarction, angina, or heart failure or who had undergone coronary revascularisation. Two reviewers independently assessed the eligibility of the identified trials and extracted data independently. Authors were contacted when possible to obtain missing information.
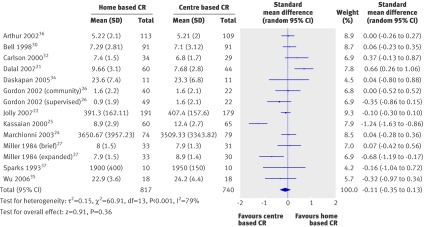
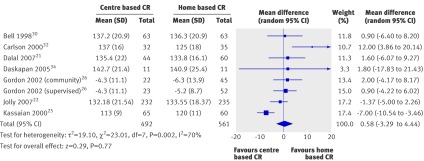
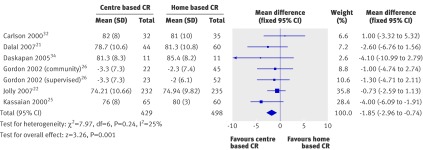
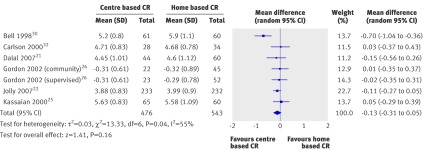
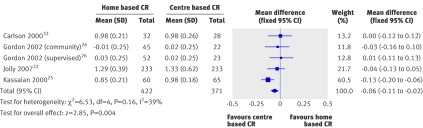
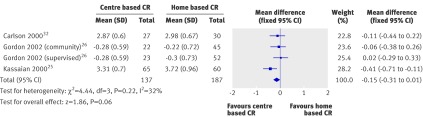
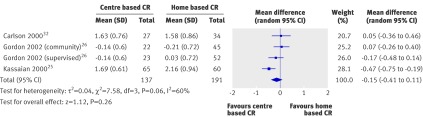
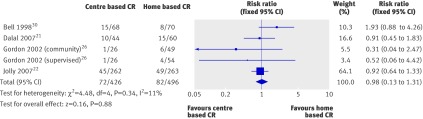
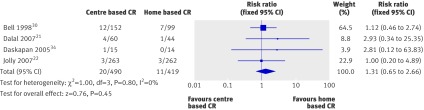
Results: 12 studies (1938 participants) were included. Most studies recruited patients with a low risk of further events after myocardial infarction or revascularisation. No difference was seen between home based and centre based cardiac rehabilitation in terms of mortality (relative risk 1.31, 95% confidence interval 0.65 to 2.66), cardiac events, exercise capacity (standardised mean difference -0.11, -0.35 to 0.13), modifiable risk factors (weighted mean difference systolic blood pressure (0.58 mm Hg, -3.29 mm Hg to 4.44 mm Hg), total cholesterol (-0.13 mmol/l, -0.31 mmol/l to 0.05 mmol/l), low density lipoprotein cholesterol (-0.15 mmol/l, -0.31 mmol/l to 0.01 mmol/l), or relative risk for proportion of smokers at follow-up (0.98, 0.73 to 1.31)), or health related quality of life, with the exception of high density lipoprotein cholesterol (-0.06, -0.11 to -0.02) mmol/l). In the home based participants, there was evidence of superior adherence. No consistent difference was seen in the healthcare costs of the two forms of cardiac rehabilitation.
Conclusions: Home and centre based forms of cardiac rehabilitation seem to be equally effective in improving clinical and health related quality of life outcomes in patients with a low risk of further events after myocardial infarction or revascularisation. This finding, together with the absence of evidence of differences in patients' adherence and healthcare costs between the two approaches, supports the further provision of evidence based, home based cardiac rehabilitation programmes such as the "Heart Manual." The choice of participating in a more traditional supervised centre based or evidence based home based programme should reflect the preference of the individual patient.
Conflict of interest statement
Competing interests: KJ was the first author of the previous systematic review of home based versus centre based cardiac rehabilitation and principal investigator of the BRUM trial of home based versus centre based cardiac rehabilitation. HD was principal investigator on the CHARMS trial of home based versus centre based cardiac rehabilitation and was invited to become an honorary medical consultant to the Heart Manual programme after this paper was submitted for publication. RST was a coauthor of the previous systematic review of home based versus centre based cardiac rehabilitation and a coinvestigator of the BRUM and CHARMS trials of home based versus centre based cardiac rehabilitation.
Figures


Comment in
-
Home based cardiac rehabilitation.BMJ. 2010 Jan 19;340:b5510. doi: 10.1136/bmj.b5510. BMJ. 2010. PMID: 20085990 No abstract available.
-
Systematic review with meta-analysis: Systematic review finds no difference between home-based and centre-based cardiac rehabilitation in terms of effect on mortality, morbidity and modifiable risk factors in patients with CHD.Evid Based Med. 2010 Apr;15(2):38. doi: 10.1136/ebm1031. Evid Based Med. 2010. PMID: 20436112 No abstract available.
-
Systematic review finds no difference in effect between home and centre-based cardiac rehabilitation on mortality, morbidity and modifiable risk factors in patients with CHD.Evid Based Nurs. 2010 Apr;13(2):38. doi: 10.1136/ebn1033. Evid Based Nurs. 2010. PMID: 20436138 No abstract available.
References
-
- Neal B. Secondary prevention of cardiovascular disease: fixed dose combinations. In: Kaplan W, Laing R, eds. Priority medicines for Europe and the world. World Health Organization, 2004.
-
- Law MR, Watt HC, Wald NJ. The underlying risk of death after myocardial infarction in the absence of treatment. Arch Intern Med 2002;162:2405-10. - PubMed
-
- World Health Organization. The world health report: conquering suffering, enriching humanity. WHO, 1997. - PubMed
-
- Jolliffe JA, Rees K, Taylor RS, Thompson D, Oldridge N, Ebrahim S. Exercise-based rehabilitation for coronary heart disease. Cochrane Database Syst Rev 2001;1:CD001800. - PubMed
-
- Taylor RS, Brown A, Ebrahim S, Jolliffe J, Noorani H, Rees K, et al. Exercise-based rehabilitation for patients with coronary heart disease: systematic review and meta-analysis of randomized controlled trials. Am J Med 2004;116:682-92. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical