

Prevalence, resistance mechanisms, and susceptibility of multidrug-resistant bloodstream isolates of Pseudomonas aeruginosa
- PMID: 20086165
- PMCID: PMC2826008
- DOI: 10.1128/AAC.01446-09
Prevalence, resistance mechanisms, and susceptibility of multidrug-resistant bloodstream isolates of Pseudomonas aeruginosa
Abstract
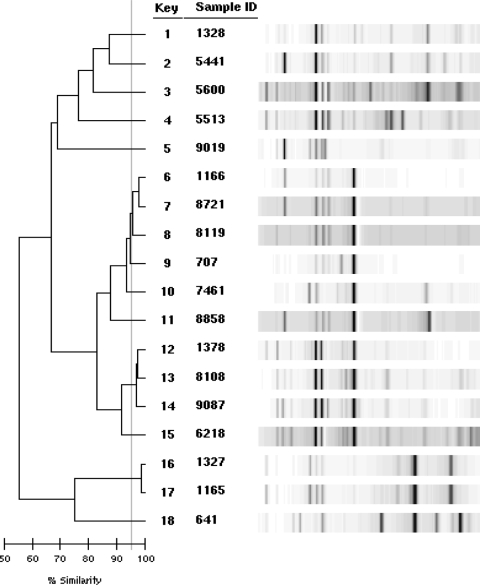
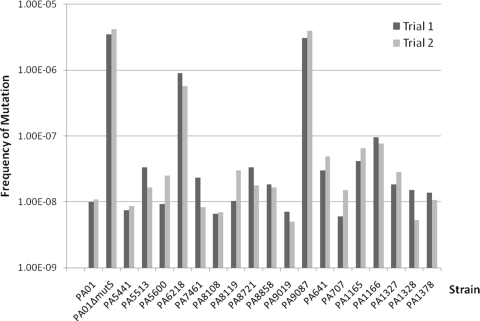
Pseudomonas aeruginosa is an important pathogen commonly implicated in nosocomial infections. The occurrence of multidrug-resistant (MDR) P. aeruginosa strains is increasing worldwide and limiting our therapeutic options. The MDR phenotype can be mediated by a variety of resistance mechanisms, and the corresponding relative biofitness is not well established. We examined the prevalence, resistance mechanisms, and susceptibility of MDR P. aeruginosa isolates (resistant to > or =3 classes of antipseudomonal agents [penicillins/cephalosporins, carbapenems, quinolones, and aminoglycosides]) obtained from a large, university-affiliated hospital. Among 235 nonrepeat bloodstream isolates screened between 2005 and 2007, 33 isolates (from 20 unique patients) were found to be MDR (crude prevalence rate, 14%). All isolates were resistant to carbapenems and quinolones, 91% were resistant to penicillins/cephalosporins, and 21% were resistant to the aminoglycosides. By using the first available isolate for each bacteremia episode (n = 18), 13 distinct clones were revealed by repetitive-element-based PCR. Western blotting revealed eight isolates (44%) to have MexB overexpression. Production of a carbapenemase (VIM-2) was found in one isolate, and mutations in gyrA (T83I) and parC (S87L) were commonly found. Growth rates of most MDR isolates were similar to that of the wild type, and two isolates (11%) were found to be hypermutable. All available isolates were susceptible to polymyxin B, and only one isolate was nonsusceptible to colistin (MIC, 3 mg/liter), but all isolates were nonsusceptible to doripenem (MIC, >2 mg/liter). Understanding and continuous monitoring of the prevalence and resistance mechanisms of MDR P. aeruginosa would enable us to formulate rational treatment strategies to combat nosocomial infections.
Figures
Similar articles
-
Prevalence, mechanisms, and risk factors of carbapenem resistance in bloodstream isolates of Pseudomonas aeruginosa.Diagn Microbiol Infect Dis. 2007 Jul;58(3):309-14. doi: 10.1016/j.diagmicrobio.2007.05.006. Diagn Microbiol Infect Dis. 2007. PMID: 17617302
-
Molecular epidemiology of Pseudomonas aeruginosa isolated from infected ICU patients: a French multicenter 2012-2013 study.Eur J Clin Microbiol Infect Dis. 2019 May;38(5):921-926. doi: 10.1007/s10096-019-03519-w. Epub 2019 Mar 2. Eur J Clin Microbiol Infect Dis. 2019. PMID: 30826996
-
Antibiotic resistance rates for Pseudomonas aeruginosa clinical respiratory and bloodstream isolates among the Veterans Affairs Healthcare System from 2009 to 2013.Diagn Microbiol Infect Dis. 2018 Apr;90(4):311-315. doi: 10.1016/j.diagmicrobio.2017.11.022. Epub 2017 Dec 6. Diagn Microbiol Infect Dis. 2018. PMID: 29310949 Free PMC article.
-
Epidemiology of Multidrug-Resistant Pseudomonas aeruginosa in the Middle East and North Africa Region.mSphere. 2021 May 19;6(3):e00202-21. doi: 10.1128/mSphere.00202-21. mSphere. 2021. PMID: 34011686 Free PMC article. Review.
-
Pseudomonas aeruginosa epidemic high-risk clones and their association with horizontally-acquired β-lactamases: 2020 update.Int J Antimicrob Agents. 2020 Dec;56(6):106196. doi: 10.1016/j.ijantimicag.2020.106196. Epub 2020 Oct 9. Int J Antimicrob Agents. 2020. PMID: 33045347 Review.
Cited by
-
Disk Carbapenemase Test for the Rapid Detection of KPC-, NDM-, and Other Metallo-β-Lactamase-Producing Gram-Negative Bacilli.Ann Lab Med. 2016 Sep;36(5):434-40. doi: 10.3343/alm.2016.36.5.434. Ann Lab Med. 2016. PMID: 27374708 Free PMC article.
-
Multidrug resistant bacteremia in hematopoietic stem cell transplant recipients.Tunis Med. 2021 Feb;99(2):269-276. Tunis Med. 2021. PMID: 33899198 Free PMC article. English.
-
Phylogenetic group, antibiotic resistance, virulence gene, and genetic diversity of Escherichia coli causing bloodstream infections in Iran.Front Microbiol. 2024 Jul 19;15:1426510. doi: 10.3389/fmicb.2024.1426510. eCollection 2024. Front Microbiol. 2024. PMID: 39101041 Free PMC article.
-
Challenges of antibacterial discovery.Clin Microbiol Rev. 2011 Jan;24(1):71-109. doi: 10.1128/CMR.00030-10. Clin Microbiol Rev. 2011. PMID: 21233508 Free PMC article. Review.
-
Effects of Polyethyelene Glycol-Desferrioxamine:Gallium Conjugates on Pseudomonas aeruginosa Outer Membrane Permeability and Vancomycin Potentiation.Mol Pharm. 2021 Feb 1;18(2):735-742. doi: 10.1021/acs.molpharmaceut.0c00820. Epub 2020 Nov 4. Mol Pharm. 2021. PMID: 33147036 Free PMC article.
References
-
- Aboufaycal, H., H. S. Sader, K. Rolston, L. M. Deshpande, M. Toleman, G. Bodey, I. Raad, and R. N. Jones. 2007. blaVIM-2 and blaVIM-7 carbapenemase-producing Pseudomonas aeruginosa isolates detected in a tertiary care medical center in the United States: report from the MYSTIC program. J. Clin. Microbiol. 45:614-615. - PMC - PubMed
-
- Akasaka, T., M. Tanaka, A. Yamaguchi, and K. Sato. 2001. Type II topoisomerase mutations in fluoroquinolone-resistant clinical strains of Pseudomonas aeruginosa isolated in 1998 and 1999: role of target enzyme in mechanism of fluoroquinolone resistance. Antimicrob. Agents Chemother. 45:2263-2268. - PMC - PubMed
-
- Bonomo, R. A., and D. Szabo. 2006. Mechanisms of multidrug resistance in Acinetobacter species and Pseudomonas aeruginosa. Clin. Infect. Dis. 43(Suppl. 2):S49-S56. - PubMed
-
- Clinical and Laboratory Standards Institute. 2007. Performance standards for antimicrobial susceptibility testing: seventeenth informational supplement. CLSI document M100-S17. Clinical and Laboratory Standards Institute, Wayne, PA.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
