

Prevalence, resistance mechanisms, and susceptibility of multidrug-resistant bloodstream isolates of Pseudomonas aeruginosa
- PMID: 20086165
- PMCID: PMC2826008
- DOI: 10.1128/AAC.01446-09
Prevalence, resistance mechanisms, and susceptibility of multidrug-resistant bloodstream isolates of Pseudomonas aeruginosa
Abstract
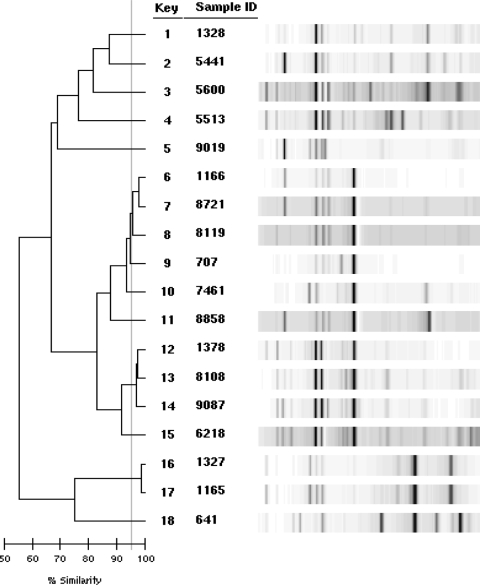
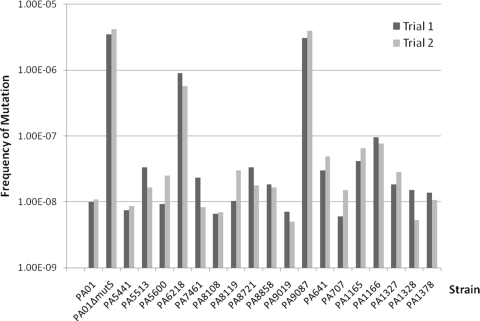
Pseudomonas aeruginosa is an important pathogen commonly implicated in nosocomial infections. The occurrence of multidrug-resistant (MDR) P. aeruginosa strains is increasing worldwide and limiting our therapeutic options. The MDR phenotype can be mediated by a variety of resistance mechanisms, and the corresponding relative biofitness is not well established. We examined the prevalence, resistance mechanisms, and susceptibility of MDR P. aeruginosa isolates (resistant to > or =3 classes of antipseudomonal agents [penicillins/cephalosporins, carbapenems, quinolones, and aminoglycosides]) obtained from a large, university-affiliated hospital. Among 235 nonrepeat bloodstream isolates screened between 2005 and 2007, 33 isolates (from 20 unique patients) were found to be MDR (crude prevalence rate, 14%). All isolates were resistant to carbapenems and quinolones, 91% were resistant to penicillins/cephalosporins, and 21% were resistant to the aminoglycosides. By using the first available isolate for each bacteremia episode (n = 18), 13 distinct clones were revealed by repetitive-element-based PCR. Western blotting revealed eight isolates (44%) to have MexB overexpression. Production of a carbapenemase (VIM-2) was found in one isolate, and mutations in gyrA (T83I) and parC (S87L) were commonly found. Growth rates of most MDR isolates were similar to that of the wild type, and two isolates (11%) were found to be hypermutable. All available isolates were susceptible to polymyxin B, and only one isolate was nonsusceptible to colistin (MIC, 3 mg/liter), but all isolates were nonsusceptible to doripenem (MIC, >2 mg/liter). Understanding and continuous monitoring of the prevalence and resistance mechanisms of MDR P. aeruginosa would enable us to formulate rational treatment strategies to combat nosocomial infections.
Figures
References
-
- Aboufaycal, H., H. S. Sader, K. Rolston, L. M. Deshpande, M. Toleman, G. Bodey, I. Raad, and R. N. Jones. 2007. blaVIM-2 and blaVIM-7 carbapenemase-producing Pseudomonas aeruginosa isolates detected in a tertiary care medical center in the United States: report from the MYSTIC program. J. Clin. Microbiol. 45:614-615. - PMC - PubMed
-
- Akasaka, T., M. Tanaka, A. Yamaguchi, and K. Sato. 2001. Type II topoisomerase mutations in fluoroquinolone-resistant clinical strains of Pseudomonas aeruginosa isolated in 1998 and 1999: role of target enzyme in mechanism of fluoroquinolone resistance. Antimicrob. Agents Chemother. 45:2263-2268. - PMC - PubMed
-
- Bonomo, R. A., and D. Szabo. 2006. Mechanisms of multidrug resistance in Acinetobacter species and Pseudomonas aeruginosa. Clin. Infect. Dis. 43(Suppl. 2):S49-S56. - PubMed
-
- Clinical and Laboratory Standards Institute. 2007. Performance standards for antimicrobial susceptibility testing: seventeenth informational supplement. CLSI document M100-S17. Clinical and Laboratory Standards Institute, Wayne, PA.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
