

Quadriceps and hamstrings muscle dysfunction after total knee arthroplasty
- PMID: 20087703
- PMCID: PMC2919870
- DOI: 10.1007/s11999-009-1219-6
Quadriceps and hamstrings muscle dysfunction after total knee arthroplasty
Abstract
Background/rationale: Although TKA reliably reduces pain from knee osteoarthritis, full recovery of muscle strength and physical function to normal levels is rare. We presumed that a better understanding of acute changes in hamstrings and quadriceps muscle performance would allow us to enhance early rehabilitation after TKA and improve long-term function.
Questions/purposes: The purposes of this study were to (1) evaluate postoperative quadriceps and hamstrings muscle strength loss after TKA and subsequent recovery using the nonoperative legs and healthy control legs for comparison, and (2) measure hamstrings coactivation before and after TKA during a maximal isometric quadriceps muscle contraction and compare with nonoperative and healthy control legs.
Methods: We prospectively followed 30 patients undergoing TKA at 2 weeks preoperatively and 1, 3, and 6 months postoperatively and compared patient outcomes with a cross-sectional cohort of 15 healthy older adults. Bilateral, isometric strength of the quadriceps and hamstrings was assessed along with EMG measures of hamstrings coactivation during a maximal isometric quadriceps contraction.
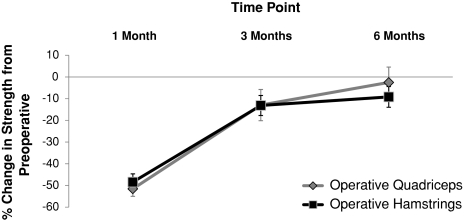
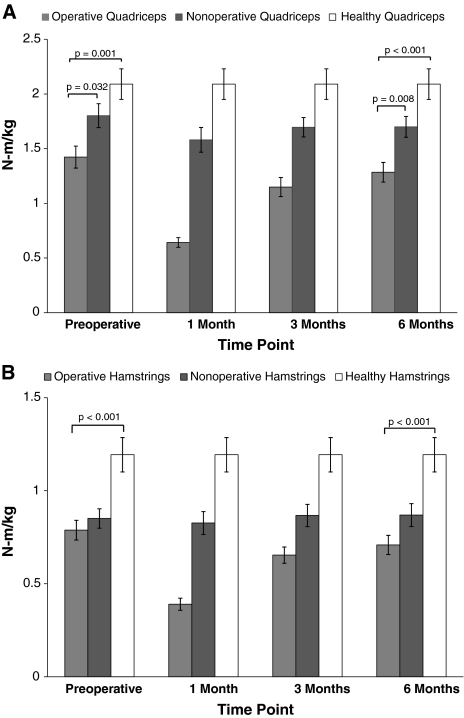
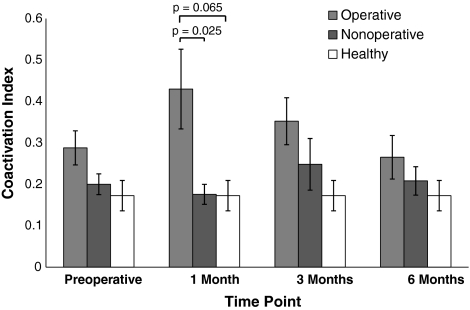
Results: There were no differences in strength loss or recovery between the quadriceps and hamstrings muscles of the operative leg throughout the followup, although differences existed when compared with nonoperative and healthy control legs. Hamstrings muscle coactivation in the operative leg during a maximal quadriceps effort was elevated at 1 month (144.5%) compared to the nonoperative leg.
Conclusions: Although quadriceps dysfunction after TKA typically is recognized and addressed in postoperative therapy protocols, hamstrings dysfunction also is present and should be addressed.
Clinical relevance: Quadriceps and hamstrings muscle strengthening should be the focus of future rehabilitation programs to optimize muscle function and long-term outcomes.
Figures
Similar articles
-
Quadriceps/hamstrings co-activation increases early after total knee arthroplasty.Knee. 2014 Dec;21(6):1115-9. doi: 10.1016/j.knee.2014.08.001. Epub 2014 Sep 11. Knee. 2014. PMID: 25218971 Free PMC article.
-
Association between long-term quadriceps weakness and early walking muscle co-contraction after total knee arthroplasty.Knee. 2013 Dec;20(6):426-31. doi: 10.1016/j.knee.2012.12.008. Epub 2013 Jan 23. Knee. 2013. PMID: 23352711 Free PMC article.
-
Does Tourniquet Use in TKA Affect Recovery of Lower Extremity Strength and Function? A Randomized Trial.Clin Orthop Relat Res. 2016 Jan;474(1):69-77. doi: 10.1007/s11999-015-4393-8. Clin Orthop Relat Res. 2016. PMID: 26100254 Free PMC article. Clinical Trial.
-
Resistance exercise training to improve post-operative rehabilitation in knee arthroplasty patients: A narrative review.Eur J Sport Sci. 2024 Jul;24(7):938-949. doi: 10.1002/ejsc.12114. Epub 2024 May 12. Eur J Sport Sci. 2024. PMID: 38956794 Free PMC article. Review.
-
The past and future of peri-operative interventions to reduce arthrogenic quadriceps muscle inhibition after total knee arthroplasty: A narrative review.Osteoarthr Cartil Open. 2023 Dec 21;6(1):100429. doi: 10.1016/j.ocarto.2023.100429. eCollection 2024 Mar. Osteoarthr Cartil Open. 2023. PMID: 38304413 Free PMC article. Review.
Cited by
-
Muscle-specific changes of lower extremities in the early period after total knee arthroplasty: Insight from tensiomyography.J Musculoskelet Neuronal Interact. 2020 Sep 1;20(3):390-397. J Musculoskelet Neuronal Interact. 2020. PMID: 32877975 Free PMC article. Clinical Trial.
-
Early Post-Operative Intervention of Whole-Body Vibration in Patients After Total Knee Arthroplasty: A Pilot Study.J Clin Med. 2019 Nov 7;8(11):1902. doi: 10.3390/jcm8111902. J Clin Med. 2019. PMID: 31703305 Free PMC article.
-
Weight-bearing radiography depends on limb loading.Knee Surg Sports Traumatol Arthrosc. 2019 May;27(5):1470-1476. doi: 10.1007/s00167-018-5056-6. Epub 2018 Jul 10. Knee Surg Sports Traumatol Arthrosc. 2019. PMID: 29992465
-
Unilateral Strength Training Imparts a Cross-Education Effect in Unilateral Knee Osteoarthritis Patients.J Funct Morphol Kinesiol. 2022 Sep 28;7(4):77. doi: 10.3390/jfmk7040077. J Funct Morphol Kinesiol. 2022. PMID: 36278738 Free PMC article.
-
Quadriceps strength impairment in the mid- to long-term follow-up period after total knee arthroplasty.Knee Surg Sports Traumatol Arthrosc. 2017 Nov;25(11):3372-3377. doi: 10.1007/s00167-016-4333-5. Epub 2016 Sep 20. Knee Surg Sports Traumatol Arthrosc. 2017. PMID: 27650527
References
-
- American Academy of Orthopaedic Surgeons. Most commonly performed musculoskeletal-related procedures. Available at: www.aaos.org/research/stats/top_hospitalization_visits.pdf. Accessed June 27, 2009.
-
- Berman AT, Bosacco SJ, Israelite C. Evaluation of total knee arthroplasty using isokinetic testing. Clin Orthop Relat Res. 1991;271:106–113. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
