

Adjuvant chemoradiation for pancreatic adenocarcinoma: the Johns Hopkins Hospital-Mayo Clinic collaborative study
- PMID: 20087786
- PMCID: PMC2840672
- DOI: 10.1245/s10434-009-0743-7
Adjuvant chemoradiation for pancreatic adenocarcinoma: the Johns Hopkins Hospital-Mayo Clinic collaborative study
Abstract
Background: Survival for pancreatic ductal adenocarcinoma is low, the role of adjuvant therapy remains controversial, and recent data suggest adjuvant chemoradiation (CRT) may decrease survival compared with surgery alone. Our goal was to examine efficacy of adjuvant CRT in resected pancreatic adenocarcinoma compared with surgery alone.
Materials and methods: Patients with pancreatic adenocarcinoma at Johns Hopkins Hospital (n = 794, 1993-2005) and Mayo Clinic (n = 478, 1985-2005) following resection who were observed (n = 509) or received adjuvant 5-FU based CRT (median dose 50.4 Gy; n = 583) were included. Cox survival and propensity score analyses assessed associations with overall survival. Matched-pair analysis by treatment group (1:1) based on institution, age, sex, tumor size/stage, differentiation, margin, and node positivity with N = 496 (n = 248 per treatment arm) was performed.
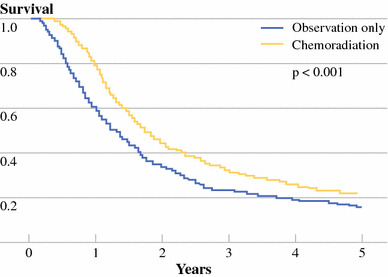
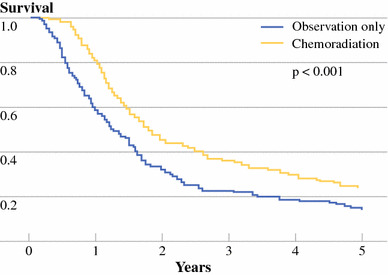
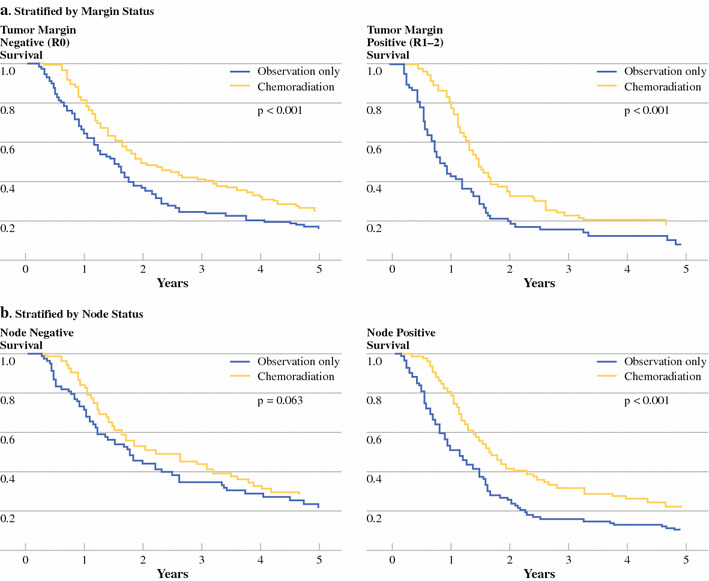
Results: Median survival was 18.8 months. Overall survival (OS) was longer among recipients of CRT versus surgery alone (median survival 21.1 vs. 15.5 months, P < .001; 2- and 5-year OS 44.7 vs. 34.6%; 22.3 vs. 16.1%, P < .001). Compared with surgery alone, adjuvant CRT improved survival in propensity score analysis for all patients by 33% (P < .001), with improved survival when stratified by age, margin, node, and T-stage (RR = 0.57-0.75, P < .05). Matched-pair analysis demonstrated OS was longer with CRT (21.9 vs. 14.3 months median survival; 2- and 5-year OS 45.5 vs. 31.4%; 25.4 vs. 12.2%, P < .001).
Conclusions: Adjuvant CRT is associated with improved survival after pancreaticoduodenectomy. Adjuvant CRT was not associated with decreased survival in any risk group, even in propensity score and matched-pair analyses. Further studies evaluating adjuvant chemotherapy compared with adjuvant chemoradiation are needed to determine the most effective combination of systemic and local-regional therapy to achieve optimal survival results.
Figures
Comment in
-
Challenges in the study of adjuvant chemoradiation after pancreaticoduodenectomy.Ann Surg Oncol. 2010 Apr;17(4):950-2. doi: 10.1245/s10434-009-0859-9. Ann Surg Oncol. 2010. PMID: 20012500 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
