

Pelvic floor consequences of cesarean delivery on maternal request in women with a single birth: a cost-effectiveness analysis
- PMID: 20088671
- PMCID: PMC2828240
- DOI: 10.1089/jwh.2009.1404
Pelvic floor consequences of cesarean delivery on maternal request in women with a single birth: a cost-effectiveness analysis
Abstract
Background: The potential benefit in preventing pelvic floor disorders (PFDs) is a frequently cited reason for requesting or performing cesarean delivery on maternal request (CDMR). However, for primigravid women without medical/obstetric indications, the lifetime cost-effectiveness of CDMR remains unknown, particularly with regard to lifelong pelvic floor consequences. Our objective was to assess the cost-effectiveness of CDMR in comparison to trial of labor (TOL) for primigravid women without medical/obstetric indications with a single childbirth over their lifetime, while explicitly accounting for the management of PFD throughout the lifetime.
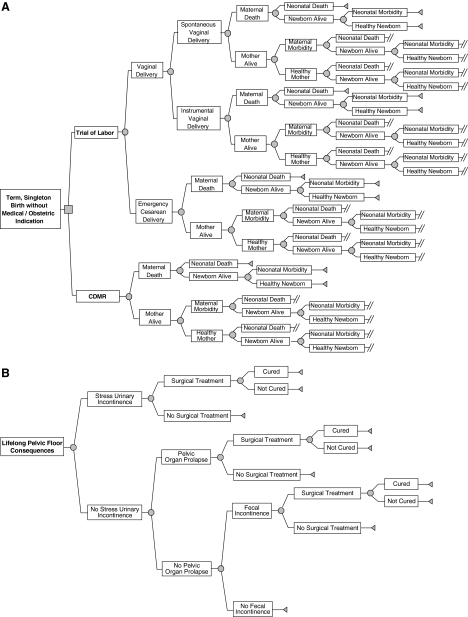
Methods: We used Monte Carlo simulation of a decision model containing 249 chance events and 101 parameters depicting lifelong maternal and neonatal outcomes in the following domains: actual mode of delivery, emergency hysterectomy, transient maternal morbidity and mortality, perinatal morbidity and mortality, and the lifelong management of PFDs. Parameter estimates were obtained from published literature. The analysis was conducted from a societal perspective. All costs and quality-adjusted life-years (QALYs) were discounted to the present value at childbirth.
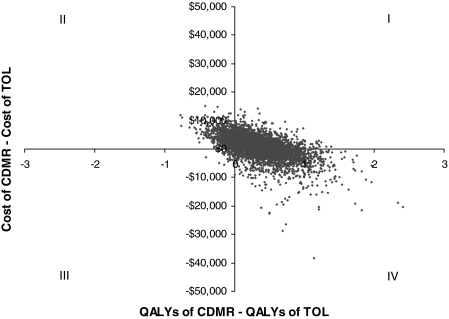
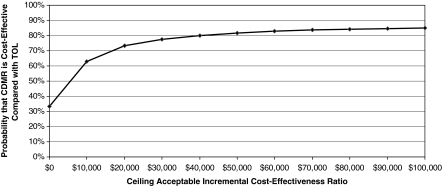
Results: The estimated mean cost and QALYs were $14,259 (95% confidence interval [CI] $8,964-$24,002) and 58.21 (95% CI 57.43-58.67) for CDMR and $13,283 (95% CI $7,861-$23,829) and 57.87 (95% CI 56.97-58.46) for TOL over the combined lifetime of the mother and the child. Parameters related to PFDs play an important role in determining cost and quality of life.
Conclusions: When a woman without medical/obstetric indications has only one childbirth in her lifetime, cost-effectiveness analysis does not reveal a clearly preferable mode of delivery.
Figures
Similar articles
-
Association of Delivery Mode With Pelvic Floor Disorders After Childbirth.JAMA. 2018 Dec 18;320(23):2438-2447. doi: 10.1001/jama.2018.18315. JAMA. 2018. PMID: 30561480 Free PMC article.
-
Role of elective cesarean section in prevention of pelvic floor disorders.Curr Opin Obstet Gynecol. 2012 Oct;24(5):318-23. doi: 10.1097/GCO.0b013e3283573fcb. Curr Opin Obstet Gynecol. 2012. PMID: 22814811 Review.
-
Comparison of pelvic floor dysfunction 6 years after uncomplicated vaginal versus elective cesarean deliveries: a cross-sectional study.Sci Rep. 2020 Dec 9;10(1):21509. doi: 10.1038/s41598-020-78625-3. Sci Rep. 2020. PMID: 33299112 Free PMC article.
-
Economic evaluation of elective cesarean versus vaginal delivery on cost of future pelvic floor disorders in the United States.Neurourol Urodyn. 2021 Jan;40(1):451-460. doi: 10.1002/nau.24582. Epub 2020 Nov 24. Neurourol Urodyn. 2021. PMID: 33232551
-
Incidence and etiology of pelvic floor dysfunction and mode of delivery: an overview.Dis Colon Rectum. 2009 Jun;52(6):1186-95. doi: 10.1007/DCR.0b013e31819f283f. Dis Colon Rectum. 2009. PMID: 19581867 Review.
Cited by
-
Simulation model of the relationship between cesarean section rates and labor duration.Health Care Manag Sci. 2019 Dec;22(4):635-657. doi: 10.1007/s10729-018-9449-3. Epub 2018 Jul 11. Health Care Manag Sci. 2019. PMID: 29995263
-
Cost-effectiveness Analysis of Intraoperative Cell Salvage for Obstetric Hemorrhage.Anesthesiology. 2018 Feb;128(2):328-337. doi: 10.1097/ALN.0000000000001981. Anesthesiology. 2018. PMID: 29194062 Free PMC article.
-
A descriptive analysis of the indications for caesarean section in mainland China.BMC Pregnancy Childbirth. 2014 Dec 12;14:410. doi: 10.1186/s12884-014-0410-2. BMC Pregnancy Childbirth. 2014. PMID: 25495550 Free PMC article.
-
Vaginal birth and pelvic floor dysfunction revisited: Can cesarean delivery be protective?Int Urogynecol J. 2016 Jan;27(1):1-2. doi: 10.1007/s00192-015-2899-y. Epub 2015 Dec 3. Int Urogynecol J. 2016. PMID: 26634838 No abstract available.
-
Cost-effectiveness of Surgical Treatment Pathways for Prolapse.Female Pelvic Med Reconstr Surg. 2021 Feb 1;27(2):e408-e413. doi: 10.1097/SPV.0000000000000948. Female Pelvic Med Reconstr Surg. 2021. PMID: 32941315 Free PMC article.
References
-
- Sakala C. Corry MP. Evidence-based maternity care: What it is and what it can achieve. New York: Childbirth Connection, Reforming States Group, Milbank Memorial Fund; 2008. [Nov 5;2008 ].
-
- ACOG Committee Opinion No. 386: Cesarean delivery on maternal request. Obstet Gynecol. 2007;110:1209–1212. - PubMed
-
- The National Institutes of Health. National Institutes of Health State-of-the-Science Conference statement: Cesarean delivery on maternal request March 27–29, 2006. Obstet Gynecol. 2006;107:1386–1397. - PubMed
-
- Hamilton BE. Martin JA. Ventura SJ. National Vital Statistics Reports, vol 56, No. 7. Hyattsville, MD: National Center for Health Statistics; 2007. Births: Preliminary data for 2006.
-
- Buhling KJ. Schmidt S. Robinson JN. Klapp C. Siebert G. Dudenhausen JW. Rate of dyspareunia after delivery in primiparae according to mode of delivery. Eur J Obstet Gynecol Reprod Biol. 2006;124:42–46. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
