

Evaluating quality of obstetric care in low-resource settings: building on the literature to design tailor-made evaluation instruments--an illustration in Burkina Faso
- PMID: 20089170
- PMCID: PMC2837005
- DOI: 10.1186/1472-6963-10-20
Evaluating quality of obstetric care in low-resource settings: building on the literature to design tailor-made evaluation instruments--an illustration in Burkina Faso
Abstract
Background: There are many instruments available freely for evaluating obstetric care quality in low-resource settings. However, this profusion can be confusing; moreover, evaluation instruments need to be adapted to local issues. In this article, we present tools we developed to guide the choice of instruments and describe how we used them in Burkina Faso to facilitate the participative development of a locally adapted instrument.
Methods: Based on a literature review, we developed two tools: a conceptual framework and an analysis grid of existing evaluation instruments. Subsequently, we facilitated several sessions with evaluation stakeholders in Burkina Faso. They used the tools to develop a locally adapted evaluation instrument that was subsequently tested in six healthcare facilities.
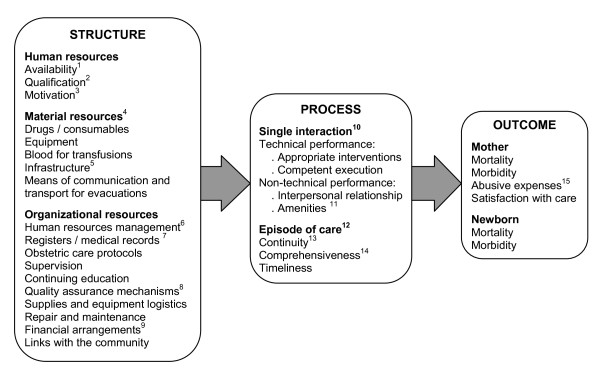
Results: Three outputs emerged from this process:1) A comprehensive conceptual framework for the quality of obstetric care, each component of which is a potential criterion for evaluation.2) A grid analyzing 37 instruments for evaluating the quality of obstetric care in low-resource settings. We highlight their key characteristics and describe how the grid can be used to prepare a new evaluation.3) An evaluation instrument adapted to Burkina Faso. We describe the experience of the Burkinabé stakeholders in developing this instrument using the conceptual framework and the analysis grid, while taking into account local realities.
Conclusions: This experience demonstrates how drawing upon existing instruments can inspire and rationalize the process of developing a new, tailor-made instrument. Two tools that came out of this experience can be useful to other teams: a conceptual framework for the quality of obstetric care and an analysis grid of existing evaluation instruments. These provide an easily accessible synthesis of the literature and are useful in integrating it with the context-specific knowledge of local actors, resulting in evaluation instruments that have both scientific and local legitimacy.
Figures
Similar articles
-
The challenges of developing an instrument to assess health provider motivation at primary care level in rural Burkina Faso, Ghana and Tanzania.Glob Health Action. 2012 Oct 1;5:1-18. doi: 10.3402/gha.v5i0.19120. Glob Health Action. 2012. PMID: 23043816 Free PMC article.
-
Maternal healthcare in context: A qualitative study of women's tactics to improve their experience of public healthcare in rural Burkina Faso.Soc Sci Med. 2015 Dec;147:98-104. doi: 10.1016/j.socscimed.2015.10.062. Epub 2015 Oct 31. Soc Sci Med. 2015. PMID: 26560408
-
Measuring self-reported health in low-income countries: piloting three instruments in semi-rural Burkina Faso.Glob Health Action. 2012;5. doi: 10.3402/gha.v5i0.8488. Epub 2012 Jul 23. Glob Health Action. 2012. PMID: 22833712 Free PMC article.
-
Local initiatives to access emergency obstetric and neonatal care in Burkina Faso.Int J Gynaecol Obstet. 2016 Nov;135 Suppl 1:S27-S32. doi: 10.1016/j.ijgo.2016.08.003. Int J Gynaecol Obstet. 2016. PMID: 27836081
-
Obstetric care in low-resource settings: what, who, and how to overcome challenges to scale up?Int J Gynaecol Obstet. 2009 Oct;107 Suppl 1:S21-44, S44-5. doi: 10.1016/j.ijgo.2009.07.017. Int J Gynaecol Obstet. 2009. PMID: 19815204 Review.
Cited by
-
Quality of perinatal care for women with high-risk pregnancies during the COVID-19 pandemic in Iran.J Int Med Res. 2022 Jul;50(7):3000605221106723. doi: 10.1177/03000605221106723. J Int Med Res. 2022. PMID: 35850546 Free PMC article.
-
Peer-driven quality improvement among health workers and traditional birth attendants in Sierra Leone: linkages between providers' organizational skills and relationships.BMC Health Serv Res. 2015;15 Suppl 1(Suppl 1):S4. doi: 10.1186/1472-6963-15-S1-S4. Epub 2015 Jun 8. BMC Health Serv Res. 2015. PMID: 26062805 Free PMC article.
-
A Framework for Describing the Influence of Service Organisation and Delivery on Participation in Fetal Anomaly Screening in England.J Pregnancy. 2017;2017:4975091. doi: 10.1155/2017/4975091. Epub 2017 Mar 22. J Pregnancy. 2017. PMID: 28421145 Free PMC article.
-
Facility-Based Maternal Quality of Care Frameworks: A Systematic Review and Best Fit Framework Analysis.Matern Child Health J. 2023 Oct;27(10):1742-1753. doi: 10.1007/s10995-023-03702-8. Epub 2023 Jul 7. Matern Child Health J. 2023. PMID: 37418097
-
Facility-Based Maternal Death in Western Africa: A Systematic Review.Front Public Health. 2018 Feb 26;6:48. doi: 10.3389/fpubh.2018.00048. eCollection 2018. Front Public Health. 2018. PMID: 29535999 Free PMC article.
References
-
- United Nations. The Millennium Development Goals Report 2007. New York: UN; 2007.
-
- World Health Organization. Maternal mortality in 2005: estimates developed by WHO, UNICEF, UNFPA, and the World Bank. Geneva: WHO; 2007.
-
- Bouvier-Colle M-H, Ouedraogo C, Dumont A, Vangeenderhuysen C, Salanave B, Decam C. Maternal mortality in West Africa. Rates, causes and substandard care from a prospective survey. Acta obstetricia et gynecologica Scandinavica. 2001;80:113–119. - PubMed
-
- World Health Organization. The world health report 2005 - make every mother and child count. Geneva: WHO; 2005.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
