

Evaluation of the optimal recall period for disease symptoms in home-based morbidity surveillance in rural and urban Kenya
- PMID: 20089695
- PMCID: PMC2846445
- DOI: 10.1093/ije/dyp374
Evaluation of the optimal recall period for disease symptoms in home-based morbidity surveillance in rural and urban Kenya
Abstract
Background: In African settings with poor access to health care, surveillance and surveys of disease burden are often done through home visits. The optimal recall period to capture data on symptoms and health utilization is unknown.
Methods: We collected illness data among 53 000 people during fortnightly home visits in rural and urban Kenya. Dates of cough, fever and diarrhoea in the past 2 weeks and health-seeking behaviour were recorded. Incidence rates were modelled using Poisson regression for data collected from 1 July 2006 to 30 June 2007.
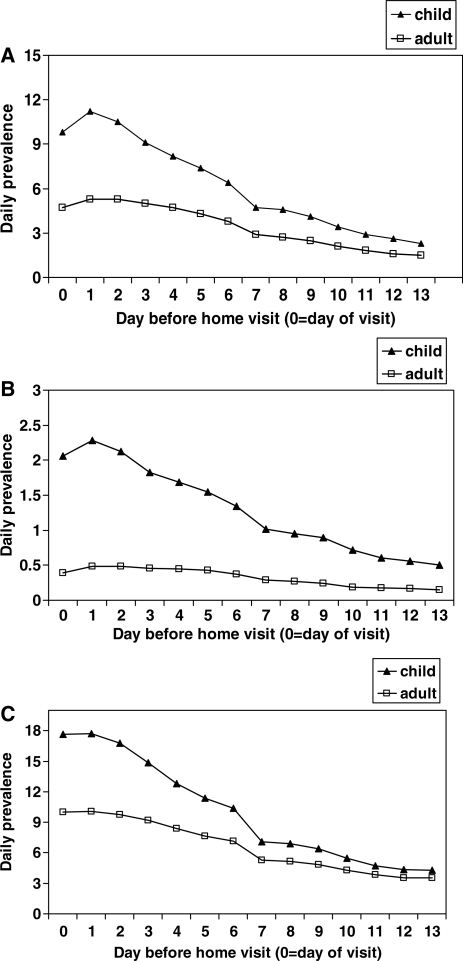
Results: Incidence rates were higher in days 0-6 before the home visit than in days 7-13 before the home visit for all three symptoms, for the rural and urban sites, for children and adults, for self- and proxy-reported symptoms and for severe and non-severe illness in children. Recall decay was steeper in the rural than the urban sites, and for proxy- than self-reported symptoms. The daily prevalence of symptoms fell <80% of the maximum prevalence when asking about symptoms >3 days before the home visit for children and >4 days for persons > or =5 years of age. Recall of previously documented clinic visits, and prescriptions of antimalarials and antibiotics also declined by approximately 7, 15 and 23% per week, respectively, in children aged <5 years, and 6, 20 and 16%, respectively, in older persons (P < 0.0001 for each decline).
Conclusions: A 2-week recall period underestimates true disease rates and health-care utilization. Shorter recall periods of 3 days in children and 4 days in adults would likely yield more accurate data.
Figures

References
-
- Amin AA, Marsh V, Noor AM, Ochola SA, Snow RW. The use of formal and informal curative services in the management of paediatric fevers in four districts in Kenya. Trop Med Int Health. 2003;8:1143–52. - PubMed
-
- Central Bureau of Statistics (CBS), Kenya Ministry of Health, ORC Macro. Kenya Demographic and Health Survey 2003: Key Findings. USA: Calverton, MD; 2004.
-
- Kroeger A. Health interview surveys in developing countries: a review of the methods and results. Int J Epidemiol. 1983;12:465–81. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
