

Computed tomographic evaluation of mouth breathers among paediatric patients
- PMID: 20089737
- PMCID: PMC3520405
- DOI: 10.1259/dmfr/80778956
Computed tomographic evaluation of mouth breathers among paediatric patients
Abstract
Objectives: Mouth breathing causes many serious problems in the paediatric population. It has been maintained that enlarged adenoids are principally responsible for mouth breathing. This study was designed to evaluate whether other mechanical obstacles might predispose the child to mouth breathing.
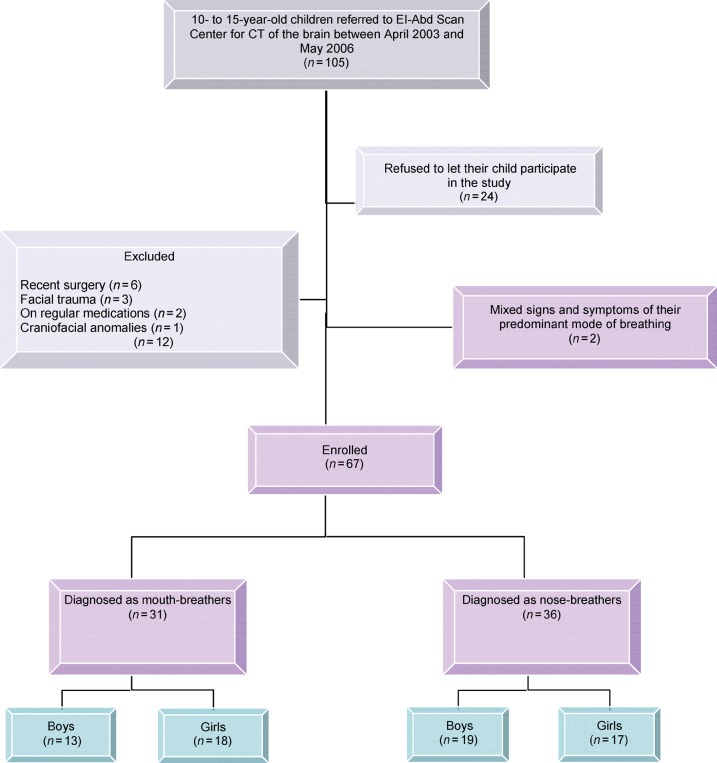
Methods: 67 children with ages ranging from 10 to 15 years were studied and grouped into mouth-breathers and nose-breathers. The children first underwent axial CT scans of the brain for which they were originally referred. In addition, they were subjected to a limited coronal CT examination of the paranasal sinuses. Congenital anatomical variations as well as inflammatory changes were assessed.
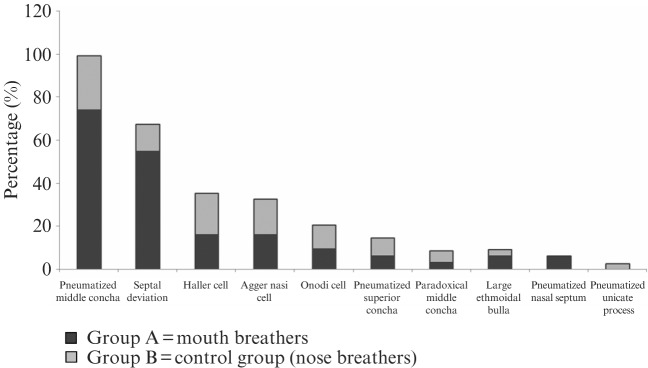
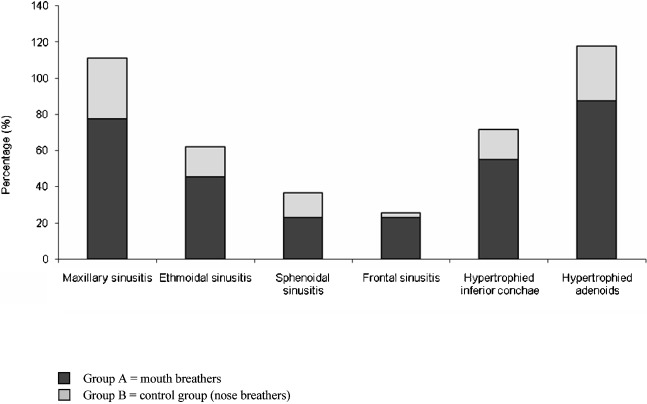
Results: 87% of mouth-breathing children had hypertrophied adenoids, 77% had maxillary sinusitis, 74% had pneumatized middle concha, 55% had a deviated nasal septum, 55% had hypertrophied inferior conchae, 45% had ethmoidal sinusitis and 23% showed frontal sinusitis. Such changes were significantly less prevalent in nose-breathers. 12.9% of mouth-breathing children did not have adenoids. Of these children, only 3.3% had one or more congenital or inflammatory change whereas the other 9.6% showed a completely normal CT scan signifying the incidence of habitual non-obstructive mouth breathing.
Conclusions: It is clear that adenoids have a dominant role in causing mouth breathing. Yet, we recommend that paediatricians should assess other mechanical obstacles if mouth breathing was not corrected after adenoidectomy. Further research should be performed to test the validity of correction of such factors in improving the quality of life of mouth-breathing children.
Figures





References
-
- Kenna MA. Nelson text book of pediatrics, 16th edn. Philadelphia, PA: WB Saunders, 2000
-
- Cattoni DM, Fernandes FD, Di Francesco RC, Latorre Mdo R. Characteristics of the stomatognathic system of mouth breathing children: anthroposcopic approach. Pro Fono 2007;19:347. - PubMed
-
- Finkelstein Y, Wexler D, Berger G, Nachmany A, Shapiro-Feinberg M, Ophir D. Anatomical basis of sleep-related breathing abnormalities in children with nasal obstruction. Arch Otolaryngol Head Neck Surg 2000;126:593–600 - PubMed
-
- Patel MR, Davidson TM. Home sleep testing in the diagnosis and treatment of sleep disordered breathing. Otolaryngol Clin North Am 2007;40:761–784 - PubMed
-
- Peltomäki T. The effect of mode of breathing on craniofacial growth: revisited. Eur J Orthod 2007;29:426–429 - PubMed
