

Prospective study of new-onset seizures presenting as status epilepticus in childhood
- PMID: 20089940
- PMCID: PMC2830921
- DOI: 10.1212/WNL.0b013e3181d0cca2
Prospective study of new-onset seizures presenting as status epilepticus in childhood
Abstract
Objective: To characterize children with new-onset seizures presenting as status epilepticus at a tertiary care children's hospital.
Methods: Prospectively collected data were reviewed from a database derived from a mandated critical care pathway. A total of 1,382 patients presented with new-onset seizures between 2001 and 2007.
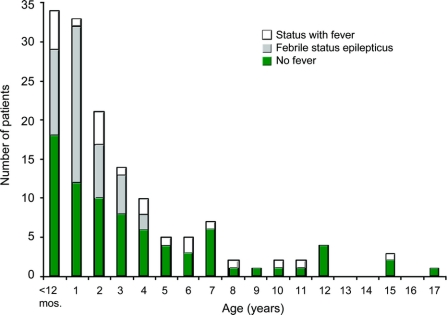
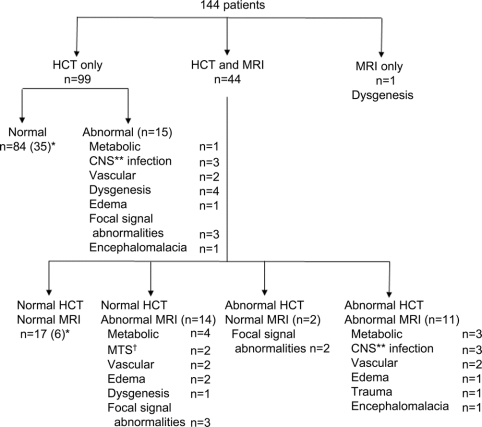
Results: A total of 144 patients presented in status epilepticus. The average age was 3.4 years. The majority of seizures (72%) lasted between 21 and 60 minutes. The majority of patients had no significant past medical history; one-fourth had a family history of epilepsy. Five (4%) patients with EEGs had electrographic seizures during the study, captured only with prolonged monitoring. The most common etiology was febrile convulsion, followed by cryptogenic. The most common acute symptomatic cause was CNS infection; the most common remote symptomatic cause was cerebral dysgenesis. Combined CT and MRI provided a diagnosis in 30%. CT was helpful in identifying acute vascular lesions and acute edema, whereas MRI was superior in identifying subtle abnormalities and remote symptomatic etiologies such as dysplasia and mesial temporal sclerosis.
Conclusions: Children who present in status epilepticus that is not a prolonged febrile convulsion should undergo neuroimaging in the initial evaluation. For any child who presents in status epilepticus and has not yet returned to baseline, the possibility of nonconvulsive status epilepticus should be considered. Although CT is often more widely accepted, especially in the urgent setting, strong consideration for MRI should be given when available, due to the superior yield.
Figures
Comment in
-
Pediatric status epilepticus: should the diagnostic evaluation change?Neurology. 2010 Feb 23;74(8):624-5. doi: 10.1212/WNL.0b013e3181d0ce5b. Epub 2010 Jan 20. Neurology. 2010. PMID: 20089938 No abstract available.
Similar articles
-
Clinical presentation of new onset refractory status epilepticus in children (the pSERG cohort).Epilepsia. 2021 Jul;62(7):1629-1642. doi: 10.1111/epi.16950. Epub 2021 Jun 6. Epilepsia. 2021. PMID: 34091885 Free PMC article.
-
Chronological Evolution of Magnetic Resonance Imaging Findings in Children With Febrile Infection-Related Epilepsy Syndrome.Pediatr Neurol. 2016 Feb;55:22-9. doi: 10.1016/j.pediatrneurol.2015.09.003. Epub 2015 Sep 25. Pediatr Neurol. 2016. PMID: 26597039
-
Mesial temporal lobe epilepsy in childhood.Epilepsia. 1996;37 Suppl 3:52-6. doi: 10.1111/j.1528-1157.1996.tb01822.x. Epilepsia. 1996. PMID: 8681915
-
The role of EEG in febrile status epilepticus (FSE).Brain Dev. 2010 Jan;32(1):37-41. doi: 10.1016/j.braindev.2009.09.015. Epub 2009 Oct 27. Brain Dev. 2010. PMID: 19864096 Review.
-
Febrile Infection-Related Epilepsy Syndrome (FIRES): A Literature Review and Case Study.Neurodiagn J. 2017;57(3):224-233. doi: 10.1080/21646821.2017.1355181. Neurodiagn J. 2017. PMID: 28898171 Review.
Cited by
-
Sociodemographic Profile, Semiology, and Etiology of Patients with Status Epilepticus: A Study from a Tertiary Care Hospital in North India.J Neurosci Rural Pract. 2018 Oct-Dec;9(4):487-491. doi: 10.4103/jnrp.jnrp_102_18. J Neurosci Rural Pract. 2018. PMID: 30271038 Free PMC article.
-
Status epilepticus and refractory status epilepticus management.Semin Pediatr Neurol. 2014 Dec;21(4):263-74. doi: 10.1016/j.spen.2014.12.006. Epub 2014 Dec 12. Semin Pediatr Neurol. 2014. PMID: 25727508 Free PMC article. Review.
-
Status epilepticus presenting as new-onset seizures in children.Epilepsy Curr. 2011 Jul;11(4):112-3. doi: 10.5698/1535-7511-11.4.112. Epilepsy Curr. 2011. PMID: 21852886 Free PMC article. No abstract available.
-
Yield of emergent neuroimaging in children with new-onset seizure and status epilepticus.Seizure. 2016 Feb;35:4-10. doi: 10.1016/j.seizure.2015.12.009. Epub 2015 Dec 25. Seizure. 2016. PMID: 26773658 Free PMC article.
-
Continuous EEG monitoring in Kenyan children with non-traumatic coma.Arch Dis Child. 2012 Apr;97(4):343-9. doi: 10.1136/archdischild-2011-300935. Epub 2012 Feb 10. Arch Dis Child. 2012. PMID: 22328741 Free PMC article.
References
-
- Chin RF, Neville BG, Peckham C, et al. Incidence, cause, and short-term outcome of convulsive status epilepticus in childhood: prospective population-based study. Lancet 2006;368:222–229. - PubMed
-
- Nishiyama I, Ohtsuka Y, Tsuda T, et al. An epidemiological study of children with status epilepticus in Okayama, Japan. Epilepsia 2007;48:1133–1137. - PubMed
-
- Wu YW, Shek DW, Garcia PA, et al. Incidence and mortality of generalized convulsive status epilepticus in California. Neurology 2002;58:1070–1076. - PubMed
-
- Hussein N, Appleton R, Thorburn K. Aetiology, course, and outcome of children admitted to paediatric intensive care with convulsive status epilepticus: a retrospective 5-year review. Seizure 2007;16:305–312. - PubMed
-
- Sillanpaa M, Shinnar S. Status epilepticus in a population-based cohort with childhood-onset epilepsy in Finland. Ann Neurol 2002;52:303–310. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous