

Caffeine for asthma
- PMID: 20091514
- PMCID: PMC7053252
- DOI: 10.1002/14651858.CD001112.pub2
Caffeine for asthma
Abstract
Background: Caffeine has a variety of pharmacological effects; it is a weak bronchodilator and it also reduces respiratory muscle fatigue. It is chemically related to the drug theophylline which is used to treat asthma. It has been suggested that caffeine may reduce asthma symptoms and interest has been expressed in its potential role as an asthma treatment. A number of studies have explored the effects of caffeine in asthma, this is the first review to systematically examine and summarise the evidence.
Objectives: To assess the effects of caffeine on lung function and identify whether there is a need to control for caffeine consumption prior to either lung function or exhaled nitric oxide testing.
Search strategy: We searched the Cochrane Airways Group trials register and the reference lists of articles (August 2009). We also contacted study authors.
Selection criteria: Randomised clinical trials of oral caffeine compared to placebo or coffee compared to decaffeinated coffee in adults with asthma.
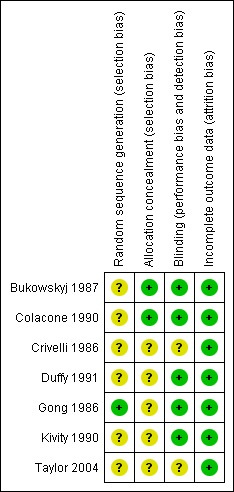
Data collection and analysis: Trial selection, quality assessment and data extraction were done independently by two reviewers.
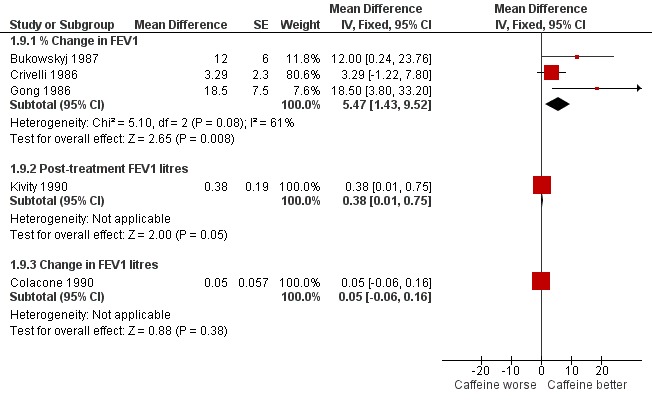
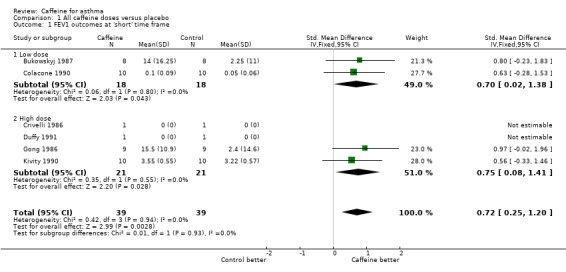
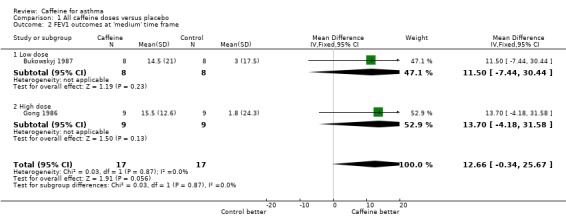
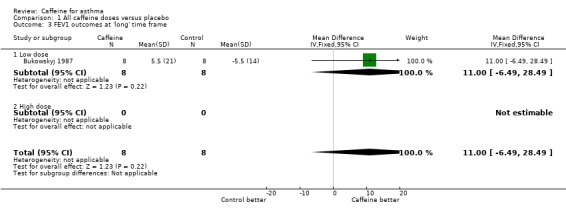
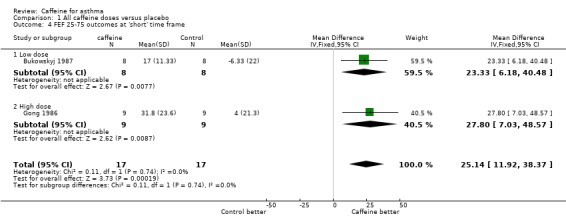
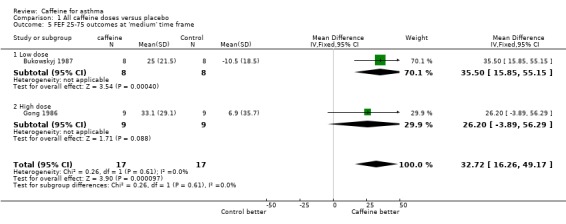
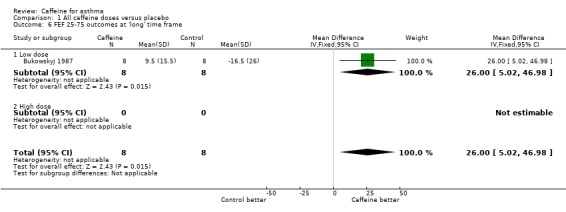
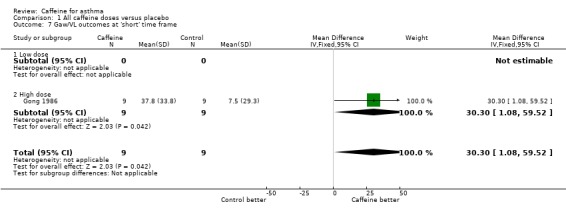
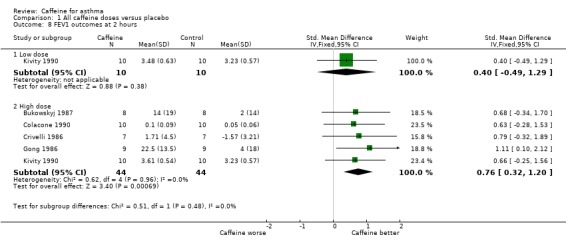
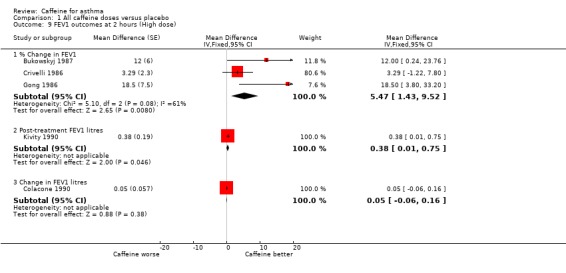
Main results: Seven trials involving a total of 75 people with mild to moderate asthma were included. The studies were all of cross-over design .Six trials involving 55 people showed that in comparison with placebo, caffeine, even at a 'low dose' (< 5mg/kg body weight), appears to improve lung function for up to two hours after consumption. Forced expiratory volume in one minute showed a small improvement up to two hours after caffeine ingestion (SMD 0.72; 95% CI 0.25 to 1.20), which translates into a 5% mean difference in FEV1. However in two studies the mean differences in FEV1 were 12% and 18% after caffeine. Mid-expiratory flow rates also showed a small improvement with caffeine and this was sustained up to four hours.One trial involving 20 people examined the effect of drinking coffee versus a decaffeinated variety on the exhaled nitric oxide levels in patients with asthma and concluded that there was no significant effect on this outcome.
Authors' conclusions: Caffeine appears to improve airways function modestly, for up to four hours, in people with asthma . People may need to avoid caffeine for at least four hours prior to lung function testing, as caffeine ingestion could cause misinterpretation of the results. Drinking caffeinated coffee before taking exhaled nitric oxide measurements does not appear to affect the results of the test, but more studies are needed to confirm this.
Conflict of interest statement
None known.
Figures
Update of
-
Caffeine for asthma.Cochrane Database Syst Rev. 2001;(4):CD001112. doi: 10.1002/14651858.CD001112. Cochrane Database Syst Rev. 2001. Update in: Cochrane Database Syst Rev. 2010 Jan 20;(1):CD001112. doi: 10.1002/14651858.CD001112.pub2. PMID: 11687099 Updated.
Similar articles
-
Caffeine for asthma.Cochrane Database Syst Rev. 2001;(4):CD001112. doi: 10.1002/14651858.CD001112. Cochrane Database Syst Rev. 2001. Update in: Cochrane Database Syst Rev. 2010 Jan 20;(1):CD001112. doi: 10.1002/14651858.CD001112.pub2. PMID: 11687099 Updated.
-
Caffeine for asthma.Cochrane Database Syst Rev. 2000;(2):CD001112. doi: 10.1002/14651858.CD001112. Cochrane Database Syst Rev. 2000. Update in: Cochrane Database Syst Rev. 2001;(4):CD001112. doi: 10.1002/14651858.CD001112. PMID: 10796597 Updated.
-
Inhaled magnesium sulfate in the treatment of acute asthma.Cochrane Database Syst Rev. 2017 Nov 28;11(11):CD003898. doi: 10.1002/14651858.CD003898.pub6. Cochrane Database Syst Rev. 2017. PMID: 29182799 Free PMC article.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2017 Dec 22;12(12):CD011535. doi: 10.1002/14651858.CD011535.pub2. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2020 Jan 9;1:CD011535. doi: 10.1002/14651858.CD011535.pub3. PMID: 29271481 Free PMC article. Updated.
Cited by
-
Impact of non-drug therapies on asthma control: A systematic review of the literature.Eur J Gen Pract. 2019 Apr;25(2):65-76. doi: 10.1080/13814788.2019.1574742. Epub 2019 Mar 8. Eur J Gen Pract. 2019. PMID: 30849253 Free PMC article.
-
Effect of Oral Caffeine on Weaning from Mechanical Ventilation in Intubated ICU Patients.Tanaffos. 2023 Feb;22(2):230-235. Tanaffos. 2023. PMID: 38628882 Free PMC article.
-
Caffeine in the Perioperative Setting.Anesthesiology. 2025 Mar 1;142(3):558-566. doi: 10.1097/ALN.0000000000005259. Epub 2025 Jan 14. Anesthesiology. 2025. PMID: 39813403
-
Evidence for lifestyle interventions in asthma.Breathe (Sheff). 2019 Jun;15(2):e50-e61. doi: 10.1183/20734735.0019-2019. Breathe (Sheff). 2019. PMID: 31777565 Free PMC article. Review.
-
The Effect of Coffee in the Prevention of Oral Mucositis Associated with Head and Neck Radiotherapy.Florence Nightingale J Nurs. 2023 Jun;31(2):105-114. doi: 10.5152/FNJN.2023.22282. Florence Nightingale J Nurs. 2023. PMID: 37404213 Free PMC article.
References
References to studies included in this review
Bukowskyj 1987 {published data only}
-
- Bukowskyj M, Nakatsu K. The bronchodilator effect of caffeine in adult asthmatics. American Review of Respiratory Disease 1987;135(1):173‐5. - PubMed
Colacone 1990 {published data only}
Crivelli 1986 {published data only}
-
- Crivelli M, Wahllander A, Jost G, Preisig R, Bachofen H. Effect of dietary caffeine on airway reactivity in asthma. Respiration 1986;50(4):258‐64. - PubMed
Duffy 1991 {published data only}
-
- Duffy P, Phillips YY. Caffeine consumption decreases the response to bronchoprovocation challenge with dry gas hyperventilation. Chest 1991;99(6):1374‐7. - PubMed
Gong 1986 {published data only}
-
- Gong H Jr, Simmons MS, Tashkin DP, Hui KK, Lee EY. Bronchodilator effects of caffeine in coffee. A dose‐response study of asthmatic subjects. Chest 1986;89(3):335‐42. - PubMed
Kivity 1990 {published data only}
-
- Kivity S, Aharon YB, Man A, Topilsky M. The effect of caffeine on exercise‐induced bronchoconstriction. Chest 1990;97(5):1083‐5. - PubMed
Taylor 2004 {published data only}
-
- Taylor E, Smith AD, Herbison GP, Cowan JO, Taylor DR. Effect of caffeine on exhaled nitric oxide measurements in asthma [Abstract]. European Respiratory Journal 2003;22(Suppl 45):P1165.
-
- Taylor ES, Smith AD, Cowan JO, Herbison GP, Taylor DR. Effect of caffeine ingestion on exhaled nitric oxide measurements in patients with asthma. American Journal of Respiratory and Critical Care Medicine 2004;169(9):1019‐21. - PubMed
References to studies excluded from this review
Becker 1984 {published data only}
-
- Becker AB, Simons KJ, Gillespie CA, Simons FE. The bronchodilator effects and pharmacokinetics of caffeine in asthma. New England Journal of Medicine 1984;310(12):743‐6. - PubMed
Henderson 1993 {published data only}
Simmons 1983 {published data only}
-
- Simmons M, Gong H, Tashkin DP, Hui K, Lee E. Bronchodilator effects of coffee in asthmatics. Chest 1983;84:332. - PubMed
References to studies awaiting assessment
Yurach 2011 {published data only}
-
- Yurach MT, Davis BE, Cockcroft DW. The effect of caffeinated coffee on airway response to methacholine and exhaled nitric oxide. Respiratory Medicine 2011;105:1606‐10. - PubMed
Additional references
Bruce 2002
Cheney 1935
-
- Cheney RH. Ventricular response in caffeine‐nicotine antagonism. Journal of Pharmacology and Experimental Therapeutics 1935;54(1):42‐52.
Curatolo 1983
-
- Curatolo PW, Robertson D. The health consequences of caffeine. Annals of Internal Medicine 1983;98(1):641‐53. - PubMed
Grollman 1930
-
- Grollman A. The action of alcohol, caffeine, and tobacco, on the cardiac output (and its related functions) of normal man. Journal of Pharmacology and Experimental Therapeutics 1930;39(3):313‐27.
Higgins 2008
-
- Higgins JPT, Green S, editors. Cochrane Handbook for Systematic Reviews of Interventions Version 5.0.1 [updated September 2008]. The Cochrane Collaboration, 2008. Available from www.cochrane‐handbook.org.
Pagano 1988
-
- Pagano R, Negri E, Decarli A, Vecchia C. Coffee drinking and prevalence of bronchial asthma. Chest 1988;94(2):386‐9. - PubMed
RevMan 5.1 [Computer program]
-
- Copenhagen, The Nordic Cochrane Centre: The Cochrane Collaboration. Review Manager (RevMan) Version 5.1. Copenhagen, The Nordic Cochrane Centre: The Cochrane Collaboration, 2011.
Robertson 1978
-
- Robertson D, Frolich JC, Carr RK, Watson JT, Hollifield JW, Shand DG, et al. Effects of caffeine on plasma renin activity, catecholamines and blood pressure. New England Journal of Medicine 1978;298:181‐6. - PubMed
Stephenson 1977
-
- Stephenson PE. Physiologic and psychotropic effects of caffeine on man. Journal of the American Dietetic Association 1977;71:240‐7. - PubMed
Woodcock 1981
-
- Woodcock AA, Gross ER, Gellert A, Shah S, Johnson M, Geddes DM. Effects of dihydrocodeine, alcohol, and caffeine on breathlessness and exercise tolerance in patients with chronic obstructive lung disease and normal blood gases. New England Journal of Medicine 1981;305:1611‐6. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical