

Perfusion quality improvement and the reduction of clinical variability
- PMID: 20092088
- PMCID: PMC4813536
Perfusion quality improvement and the reduction of clinical variability
Abstract
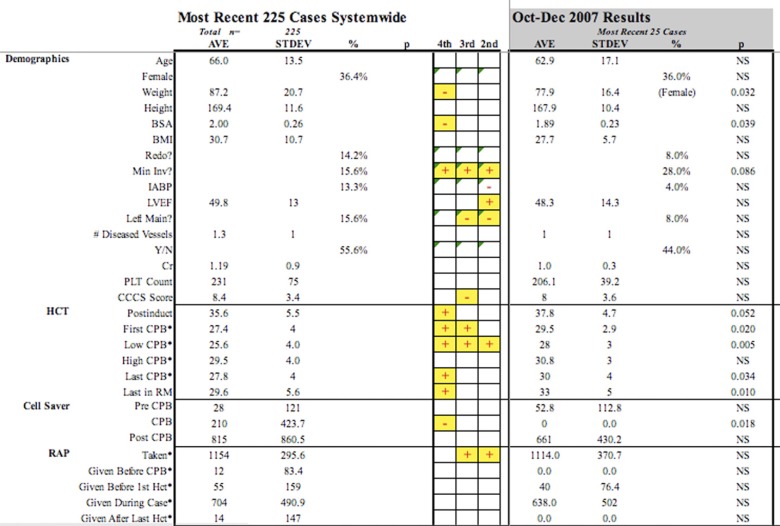
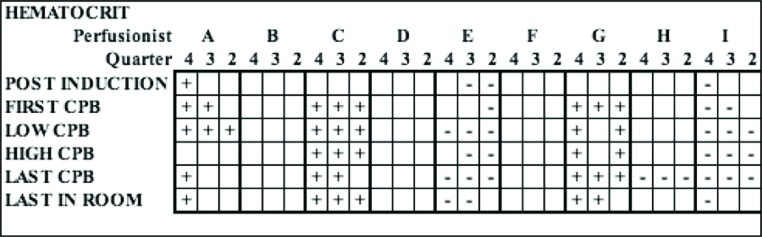
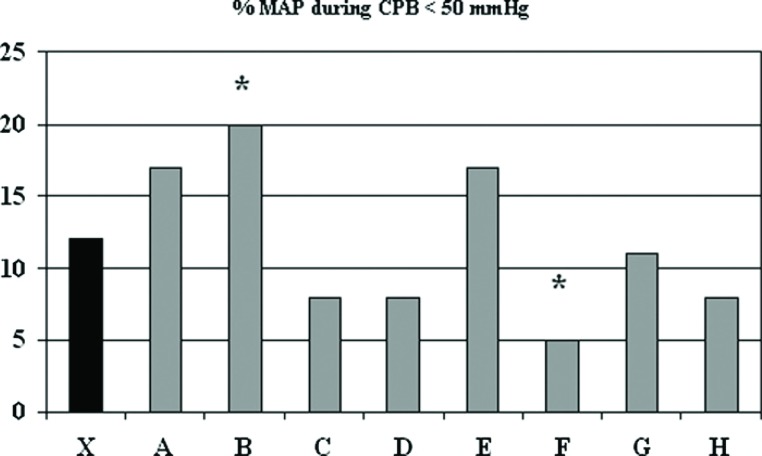
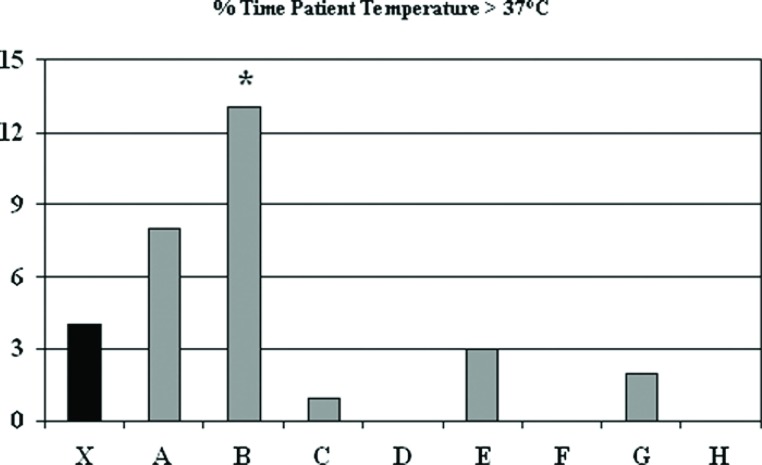
The purpose of this study was to describe the development and utilization of a perfusion quality improvement program to reduce perfusion-to-perfusion variability in a large multi-center perfusion practice. Phase I of the study included the establishment of a perfusion database using standard spreadsheet format to serve multiple administrative functions including patient and procedure sequencing, predictive algorithms for yearly caseload, summary statistics, and inter-perfusionist comparison. The database used 236 separate variables, including demographic and clinical procedure-related categories. Forty of these variables are modifiable by perfusion interaction as established via protocol and algorithm. Phase II of the study used a perfusion electronic data recording system to automatically obtain patient data from physiologic monitors and the heart-lung machine. Data were transferred to a central database for perfusionist comparison. Data analysis used logical functions and macros programming, and statistical analysis used both parametric and non-parametric models within the program. Each quarter all variables underwent analysis with summary data established for the most recent 225 patients undergoing CPB. Twenty-five cases from each perfusionist (n = 9) were compared with the aggregate data of the entire staff, with reference to previous quarter's summary statistics. The results were discussed in monthly staff meetings and methods for improving compliance were discussed. Individual variation (p < .01) varied in 17 of 40 variables (26.0 +/- 8.6), with quarterly improvement (27.4 +/- 2.3 vs. 24.2 +/- 2.1 vs. 17.0 +/- 2.1) demonstrated in seven of nine individuals. In Phase II, performance was analyzed using the same variables as in Phase I but it also included the electronically recorded data from which 27 core measures were derived. All results were discussed with the staff at monthly departmental quality improvement meetings. The perfusion quality improvement program has evolved from a simple descriptive listing of cases to a quantitative instrument used to reduce variability amongst perfusionists and assure compliance with policies and standards of care.
Figures
Similar articles
-
Getting it right: optimizing the patient and technique for the procedure.J Extra Corpor Technol. 2009 Dec;41(4):P59-64. J Extra Corpor Technol. 2009. PMID: 20092089 Free PMC article.
-
Developing a benchmarking process in perfusion: a report of the Perfusion Downunder Collaboration.J Extra Corpor Technol. 2012 Mar;44(1):26-33. J Extra Corpor Technol. 2012. PMID: 22730861 Free PMC article.
-
Improving the patient experience by improving performance: the Six Sigma way.AMIA Annu Symp Proc. 2008 Nov 6:1246. AMIA Annu Symp Proc. 2008. PMID: 18999028 No abstract available.
-
The Geat Britain and Ireland perspective: current perfusion safety issues, preparing for the future.Perfusion. 2005 Jul;20(4):217-25. doi: 10.1191/0267659105pf810oa. Perfusion. 2005. PMID: 16130368 Review.
-
Designing an integrated extracorporeal therapy service quality system.Ther Apher. 2002 Aug;6(4):282-7. doi: 10.1046/j.1526-0968.2002.00440.x. Ther Apher. 2002. PMID: 12164797 Review.
Cited by
-
2019 EACTS/EACTA/EBCP guidelines on cardiopulmonary bypass in adult cardiac surgery.Interact Cardiovasc Thorac Surg. 2020 Feb 1;30(2):161-202. doi: 10.1093/icvts/ivz251. Interact Cardiovasc Thorac Surg. 2020. PMID: 31576402 Free PMC article. No abstract available.
-
Integration of Electronic Perfusion Data for Perfusion Registries.J Extra Corpor Technol. 2018 Jun;50(2):102-112. J Extra Corpor Technol. 2018. PMID: 29921989 Free PMC article.
-
Prescriptive patient extracorporeal circuit and oxygenator sizing reduces hemodilution and allogeneic blood product transfusion during adult cardiac surgery.J Extra Corpor Technol. 2013 Sep;45(3):167-72. J Extra Corpor Technol. 2013. PMID: 24303598 Free PMC article.
-
Does Standardizing Extracorporeal Circuit Design for Cardiopulmonary Bypass Affect Outcomes? Results from a National Perfusion Registry.J Extra Corpor Technol. 2019 Dec;51(4):210-220. doi: 10.1182/ject-1900012. J Extra Corpor Technol. 2019. PMID: 31915404 Free PMC article.
-
The Effect of Standardizing Autologous Prime Techniques in Patients Undergoing Cardiac Surgery with Cardiopulmonary Bypass.J Extra Corpor Technol. 2019 Dec;51(4):227-237. doi: 10.1182/ject-1900016. J Extra Corpor Technol. 2019. PMID: 31915406 Free PMC article.
References
-
- Hosford SB.. Hospital progress in reducing error: The impact of external interventions. Hosp Top. 2008;86:9–20. - PubMed
-
- Miller MR, Pronovost P, Donithan M, et al. . Relationship between performance measurement and accreditation: Implications for quality of care and patient safety. Am J Med Qual. 2005;20:239–52. - PubMed
-
- Longo DR, Hewett JE, Ge B, Schubert S.. Hospital patient safety: Characteristics of best-performing hospitals. J Healthc Manag. 2007;52:188–204. - PubMed
-
- Jacobs JP, Mavroudis C, Jacobs ML, et al. . Nomenclature and databases—The past, the present, and the future: A primer for the congenital heart surgeon. Pediatr Cardiol. 2007;28:105–15. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical