

Ruling out coronary heart disease in primary care patients with chest pain: a clinical prediction score
- PMID: 20092615
- PMCID: PMC2832616
- DOI: 10.1186/1741-7015-8-9
Ruling out coronary heart disease in primary care patients with chest pain: a clinical prediction score
Abstract
Background: Chest pain raises concern for the possibility of coronary heart disease. Scoring methods have been developed to identify coronary heart disease in emergency settings, but not in primary care.
Methods: Data were collected from a multicenter Swiss clinical cohort study including 672 consecutive patients with chest pain, who had visited one of 59 family practitioners' offices. Using delayed diagnosis we derived a prediction rule to rule out coronary heart disease by means of a logistic regression model. Known cardiovascular risk factors, pain characteristics, and physical signs associated with coronary heart disease were explored to develop a clinical score. Patients diagnosed with angina or acute myocardial infarction within the year following their initial visit comprised the coronary heart disease group.
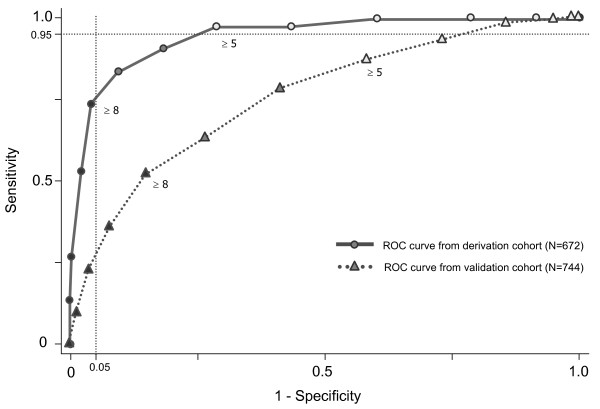
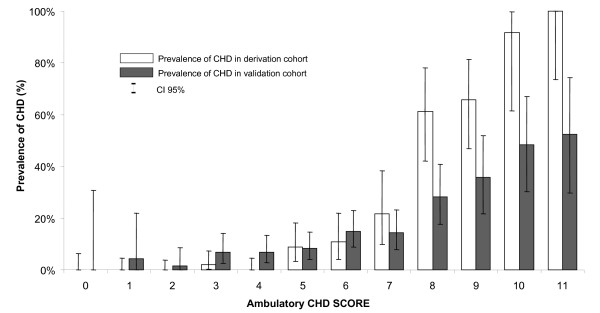
Results: The coronary heart disease score was derived from eight variables: age, gender, duration of chest pain from 1 to 60 minutes, substernal chest pain location, pain increasing with exertion, absence of tenderness point at palpation, cardiovascular risks factors, and personal history of cardiovascular disease. Area under the receiver operating characteristics curve was of 0.95 with a 95% confidence interval of 0.92; 0.97. From this score, 413 patients were considered as low risk for values of percentile 5 of the coronary heart disease patients. Internal validity was confirmed by bootstrapping. External validation using data from a German cohort (Marburg, n = 774) revealed a receiver operating characteristics curve of 0.75 (95% confidence interval, 0.72; 0.81) with a sensitivity of 85.6% and a specificity of 47.2%.
Conclusions: This score, based only on history and physical examination, is a complementary tool for ruling out coronary heart disease in primary care patients complaining of chest pain.
Figures
Similar articles
-
Development and validation of a clinical prediction rule for chest wall syndrome in primary care.BMC Fam Pract. 2012 Aug 6;13:74. doi: 10.1186/1471-2296-13-74. BMC Fam Pract. 2012. PMID: 22866824 Free PMC article.
-
Ruling out coronary artery disease in primary care: development and validation of a simple prediction rule.CMAJ. 2010 Sep 7;182(12):1295-300. doi: 10.1503/cmaj.100212. Epub 2010 Jul 5. CMAJ. 2010. PMID: 20603345 Free PMC article.
-
Ruling out coronary heart disease in primary care: external validation of a clinical prediction rule.Br J Gen Pract. 2012 Jun;62(599):e415-21. doi: 10.3399/bjgp12X649106. Br J Gen Pract. 2012. PMID: 22687234 Free PMC article.
-
[Chest pain syndrome in normal or non-diagnostic conventional ECG at the emergency service. Assessment with myocardial perfusion (SPECT) and ventricular function (Gated-SPECT)].Arch Cardiol Mex. 2004 Jan-Mar;74 Suppl 1:S18-31. Arch Cardiol Mex. 2004. PMID: 15216744 Review. Spanish.
-
HEART Score Risk Stratification of Low-Risk Chest Pain Patients in the Emergency Department: A Systematic Review and Meta-Analysis.Ann Emerg Med. 2019 Aug;74(2):187-203. doi: 10.1016/j.annemergmed.2018.12.010. Epub 2019 Feb 2. Ann Emerg Med. 2019. PMID: 30718010
Cited by
-
Clinical assessment of patients with chest pain; a systematic review of predictive tools.BMC Cardiovasc Disord. 2016 Jan 20;16:18. doi: 10.1186/s12872-016-0196-4. BMC Cardiovasc Disord. 2016. PMID: 26790953 Free PMC article.
-
Development and validation of a clinical prediction rule for chest wall syndrome in primary care.BMC Fam Pract. 2012 Aug 6;13:74. doi: 10.1186/1471-2296-13-74. BMC Fam Pract. 2012. PMID: 22866824 Free PMC article.
-
The diagnosis of coronary heart disease in a low-prevalence setting: follow-up data from patients whose CHD was misdiagnosed by their family doctors.Dtsch Arztebl Int. 2011 Jul;108(26):445-51. doi: 10.3238/arztebl.2011.0445. Epub 2011 Jul 1. Dtsch Arztebl Int. 2011. PMID: 21776318 Free PMC article.
-
Performance of the coronary calcium score in an outpatient chest pain clinic and strategies for risk stratification.Clin Cardiol. 2021 Sep;44(9):1189. doi: 10.1002/clc.23611. Epub 2021 May 12. Clin Cardiol. 2021. PMID: 33977524 Free PMC article. No abstract available.
-
An exercise programme for community-dwelling, mobility-restricted and chronically ill older adults with structured support by the general practitioner's practice (HOMEfit). From feasibility to evaluation.Z Gerontol Geriatr. 2013 Jan;46(1):56, 58-63. doi: 10.1007/s00391-012-0329-z. Z Gerontol Geriatr. 2013. PMID: 22538790 Clinical Trial.
References
-
- Luepker RV, Apple FS, Christenson RH, Crow RS, Fortmann SP, Goff D, Goldberg RJ, Hand MM, Jaffe AS, Julian DG, Levy D, Manolio T, Mendis S, Mensah G, Pajak A, Prineas RJ, Reddy KS, Roger VL, Rosamond WD, Shahar E, Sharrett AR, Sorlie P, Tunstall-Pedoe H. AHA Council on Epidemiology and Prevention; AHA Statistics Committee; World Heart Federation Council on Epidemiology and Prevention; European Society of Cardiology Working Group on Epidemiology and Prevention; Centers for Disease Control and Prevention; National Heart, Lung, and Blood Institute. Case definitions for acute coronary heart disease in epidemiology and clinical research studies: a statement from the AHA Council on Epidemiology and Prevention; AHA Statistics Committee; World Heart Federation Council on Epidemiology and Prevention; the European Society of Cardiology Working Group on Epidemiology and Prevention; Centers for Disease Control and Prevention; and the National Heart, Lung, and Blood Institute. Circulation. 2003;108:2543–2549. doi: 10.1161/01.CIR.0000100560.46946.EA. - DOI - PubMed
-
- Verdon F, Herzig L, Burnand B, Bischoff T, Pecoud A, Junod M, Muhlemann N, Favrat B. Chest pain in daily practice: occurrence, causes and management. Swiss Med Wkly. 2008;138:340–347. - PubMed
-
- Snow V, Barry P, Fihn SD, Gibbons RJ, Owens DK, Williams SV, Weiss KB, Mottur-Pilson C. Evaluation of primary care patients with chronic stable angina: guidelines from the American College of Physicians. Ann Intern Med. 2004;141:57–64. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
