

Isolated acute nontraumatic cortical subarachnoid hemorrhage
- PMID: 20093311
- PMCID: PMC7966116
- DOI: 10.3174/ajnr.A1986
Isolated acute nontraumatic cortical subarachnoid hemorrhage
Abstract
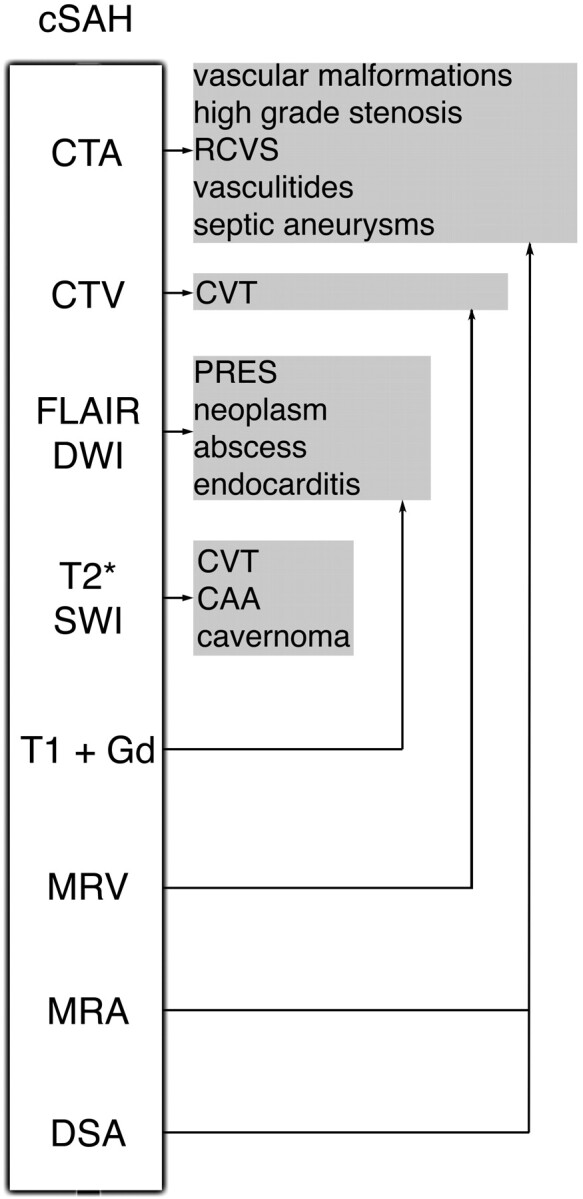
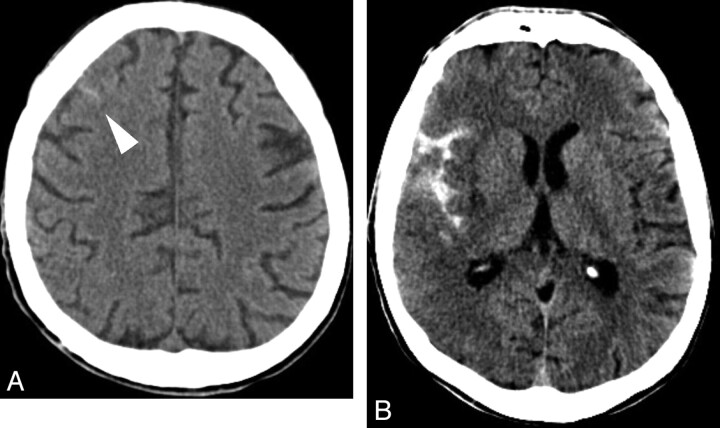
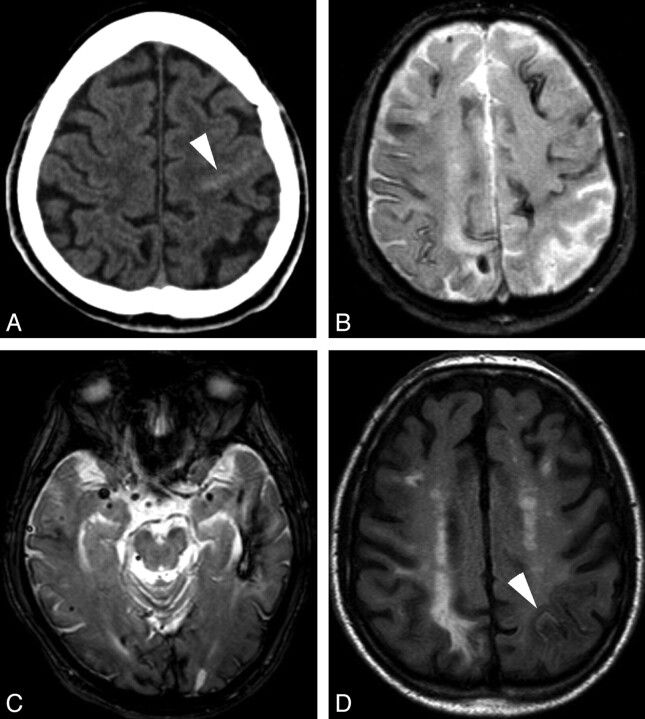
Our aim was to review the etiologic background of isolated acute nontraumatic cSAH. While SAH located in the basal cisterns originates from a ruptured aneurysm in approximately 85% of cases, a broad spectrum of vascular and even nonvascular pathologies can cause acute nontraumatic SAH along the convexity. Arteriovenous malformations or fistulas, cortical venous and/or dural sinus thrombosis, and distal and proximal arteriopathies (RCVS, vasculitides, mycotic aneurysms, Moyamoya, or severe atherosclerotic carotid disease) should be sought by noninvasive imaging methods or/and conventional angiography. Additionally, PRES may also be a source of acute cSAH. In elderly patients, cSAH might be attributed to CAA if numerous hemorrhages are demonstrated by GRE T2 images. Finally, cSAH is rarely observed in nonvascular disorders, such as abscess and primitive or secondary brain tumors.
Figures


Comment in
-
Extracranial internal carotid artery stenosis as a cause of cortical subarachnoid hemorrhage.AJNR Am J Neuroradiol. 2011 Mar;32(3):E51-2; author reply E53. doi: 10.3174/ajnr.A2456. Epub 2011 Feb 24. AJNR Am J Neuroradiol. 2011. PMID: 21349955 Free PMC article. No abstract available.
Similar articles
-
Extracranial internal carotid artery stenosis as a cause of cortical subarachnoid hemorrhage.AJNR Am J Neuroradiol. 2011 Mar;32(3):E51-2; author reply E53. doi: 10.3174/ajnr.A2456. Epub 2011 Feb 24. AJNR Am J Neuroradiol. 2011. PMID: 21349955 Free PMC article. No abstract available.
-
Nontraumatic convexity subarachnoid hemorrhage: different etiologies and outcomes.J Stroke Cerebrovasc Dis. 2014 Jan;23(1):e23-30. doi: 10.1016/j.jstrokecerebrovasdis.2013.08.005. Epub 2013 Oct 8. J Stroke Cerebrovasc Dis. 2014. PMID: 24119619
-
The Spectrum of Nontraumatic Convexity Subarachnoid Hemorrhage.J Stroke Cerebrovasc Dis. 2019 Dec;28(12):104473. doi: 10.1016/j.jstrokecerebrovasdis.2019.104473. Epub 2019 Oct 31. J Stroke Cerebrovasc Dis. 2019. PMID: 31677961
-
Convexity Subarachnoid Hemorrhage with PiB Positive Pet Scans: Clinical Features and Prognosis.J Neuroimaging. 2015 May-Jun;25(3):420-9. doi: 10.1111/jon.12188. Epub 2014 Dec 18. J Neuroimaging. 2015. PMID: 25523388 Review.
-
Midterm Follow-Up of 20 Consecutive Patients with Nonaneurysmal Subarachnoid Hemorrhage of Unknown Origin in a Single-Center: Two Cases of De Novo Development of Dural Arteriovenous Fistula.J Stroke Cerebrovasc Dis. 2017 Dec;26(12):2788-2792. doi: 10.1016/j.jstrokecerebrovasdis.2017.06.061. Epub 2017 Aug 10. J Stroke Cerebrovasc Dis. 2017. PMID: 28802521 Review.
Cited by
-
Convexal Subarachnoid Hemorrhage Caused by Infective Endocarditis in a Patient with Advanced Human Immunodeficiency Virus (HIV): The Culprits and Bystanders.Am J Case Rep. 2021 May 14;22:e931376. doi: 10.12659/AJCR.931376. Am J Case Rep. 2021. PMID: 33986239 Free PMC article.
-
Clinical and Imaging Characteristics in Patients with SARS-CoV-2 Infection and Acute Intracranial Hemorrhage.J Clin Med. 2020 Aug 6;9(8):2543. doi: 10.3390/jcm9082543. J Clin Med. 2020. PMID: 32781623 Free PMC article.
-
Non-aneurysmal spontaneous subarachnoid hemorrhage: perimesencephalic versus non-perimesencephalic.Rev Bras Ter Intensiva. 2016 Jun;28(2):141-6. doi: 10.5935/0103-507X.20160028. Rev Bras Ter Intensiva. 2016. PMID: 27410409 Free PMC article.
-
Focal subarachnoid haemorrhage mimicking transient ischaemic attack--do we really need MRI in the acute stage?BMC Neurol. 2014 Apr 10;14:80. doi: 10.1186/1471-2377-14-80. BMC Neurol. 2014. PMID: 24720867 Free PMC article.
-
Cavernous angioma presenting with subarachnoid hemorrhage which was diffusely distributed in the basal cisterns and mimicked intracranial aneurysm rupture.Surg Neurol Int. 2017 Aug 22;8:202. doi: 10.4103/sni.sni_210_17. eCollection 2017. Surg Neurol Int. 2017. PMID: 28904829 Free PMC article. No abstract available.
References
-
- van Gijn J, Rinkel GJ. Subarachnoid haemorrhage: diagnosis, causes and management. Brain 2001;124(pt 2):249–78 - PubMed
-
- Spitzer C, Mull M, Rohde V, et al. . Non-traumatic cortical subarachnoid haemorrhage: diagnostic work-up and aetiological background. Neuroradiology 2005;47:525–31. Epub 2005 Jun 22 - PubMed
-
- Patel KC, Finelli PF. Nonaneurysmal convexity subarachnoid hemorrhage. Neurocrit Care 2006;4:229–33 - PubMed
-
- Refai D, Botros JA, Strom RG, et al. . Spontaneous isolated convexity subarachnoid hemorrhage: presentation, radiological findings, differential diagnosis, and clinical course. J Neurosurg 2008;109:1034–41 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical