

High-resolution 3D MR imaging of the trochlear nerve
- PMID: 20093316
- PMCID: PMC7963936
- DOI: 10.3174/ajnr.A1992
High-resolution 3D MR imaging of the trochlear nerve
Abstract
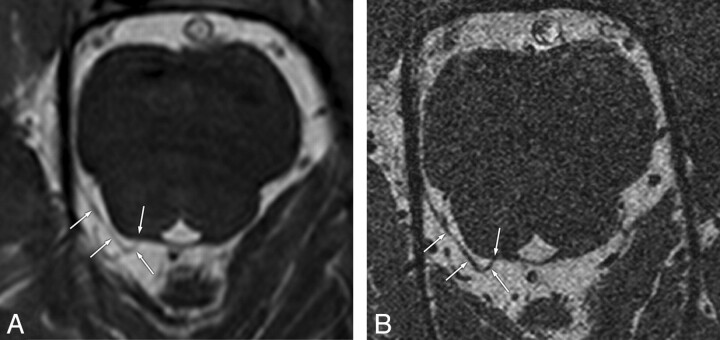
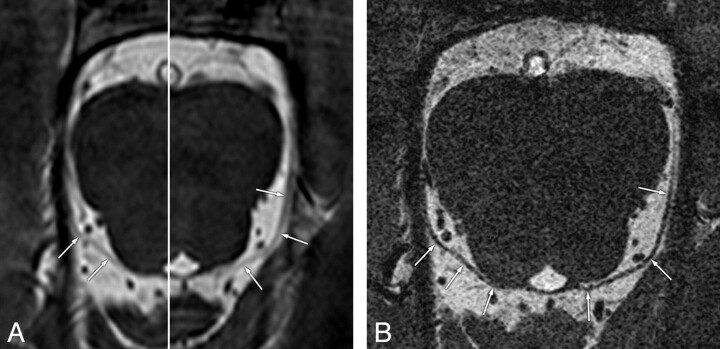
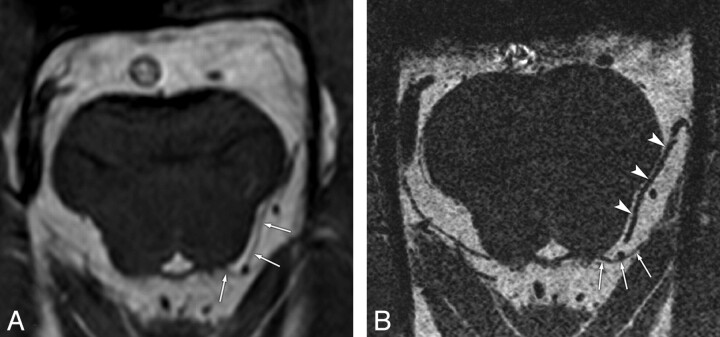
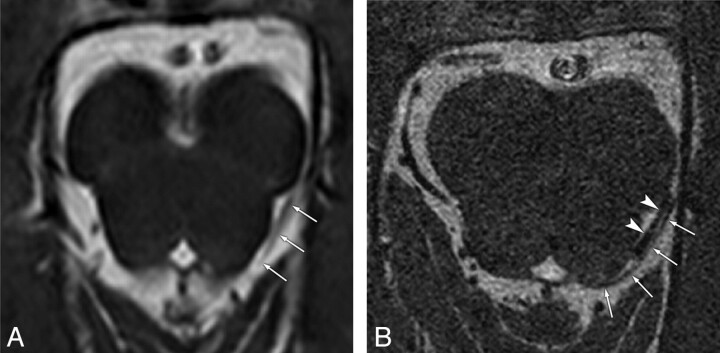
Background and purpose: The cisternal segment of the trochlear nerve is difficult to identify reliably by routine MR imaging. We investigated the visibility and anatomic features of the trochlear nerve by using high-resolution 3D-bTFE imaging in healthy subjects.
Materials and methods: This study was conducted with 32 healthy subjects without ocular movement disorders. For us to visualize the cisternal segment of the trochlear nerve, all subjects underwent 3D-bTFE imaging at 3T with 2 different resolutions: conventional resolution (voxel size, 0.67 x 0.45 x 1.4 mm) and high resolution (voxel size, 0.3 x 0.3 x 0.25 mm). Visibility of the trochlear nerve was graded with the use of a qualitative scale of certainty as follows: definite, probable, and indeterminate. The diameter of the trochlear nerve was measured.
Results: On conventional-resolution images, the visibility of the trochlear nerve was definite in 3 nerves, probable in 12 nerves, and indeterminate in 49 nerves. On high-resolution images, visibility was definite in 63 nerves and probable in 1 nerve. The mean diameter of the trochlear nerve was 0.54 mm (range, 0.35-0.96 mm).
Conclusions: The trochlear nerve was visualized 100% of the time on high-resolution imaging with a voxel smaller than the nerve diameter. High-resolution imaging should have an important role in investigating the pathogenic mechanism of neuropathic strabismus, such as congenital superior oblique palsy.
Figures
Similar articles
-
High-Resolution 7T MR Imaging of the Trochlear Nerve.AJNR Am J Neuroradiol. 2023 Feb;44(2):186-191. doi: 10.3174/ajnr.A7774. Epub 2023 Jan 19. AJNR Am J Neuroradiol. 2023. PMID: 36657953 Free PMC article.
-
Association of superior oblique muscle volumes with the presence or absence of the trochlear nerve on high-resolution MR imaging in congenital superior oblique palsy.AJNR Am J Neuroradiol. 2015 Apr;36(4):774-8. doi: 10.3174/ajnr.A4202. Epub 2015 Jan 2. AJNR Am J Neuroradiol. 2015. PMID: 25556205 Free PMC article.
-
MR anatomy of the proximal cisternal segment of the trochlear nerve: neurovascular relationships and landmarks.Radiology. 2002 Apr;223(1):31-8. doi: 10.1148/radiol.2231010612. Radiology. 2002. PMID: 11930045
-
Imaging of Cranial Nerves III, IV, VI in Congenital Cranial Dysinnervation Disorders.Korean J Ophthalmol. 2017 Jun;31(3):183-193. doi: 10.3341/kjo.2017.0024. Epub 2017 May 12. Korean J Ophthalmol. 2017. PMID: 28534340 Free PMC article. Review.
-
Central trochlear palsy.Surv Ophthalmol. 1986 Mar-Apr;30(5):279-97. doi: 10.1016/0039-6257(86)90061-5. Surv Ophthalmol. 1986. PMID: 3520909 Review.
Cited by
-
Surgical Outcomes of Inferior Oblique Myectomy in Unilateral Congenital Superior Oblique Palsy with or without Trochlear Nerve.PLoS One. 2016 Jul 8;11(7):e0156872. doi: 10.1371/journal.pone.0156872. eCollection 2016. PLoS One. 2016. PMID: 27391445 Free PMC article.
-
Magnetic resonance imaging of cranial nerves at 7 Tesla.Clin Neuroradiol. 2013 Mar;23(1):17-23. doi: 10.1007/s00062-012-0144-3. Epub 2012 Sep 27. Clin Neuroradiol. 2013. PMID: 23015059
-
High-Resolution 7T MR Imaging of the Trochlear Nerve.AJNR Am J Neuroradiol. 2023 Feb;44(2):186-191. doi: 10.3174/ajnr.A7774. Epub 2023 Jan 19. AJNR Am J Neuroradiol. 2023. PMID: 36657953 Free PMC article.
-
Characteristics of Facial Asymmetry in Congenital Superior Oblique Palsy according to Trochlear Nerve Absence.J Ophthalmol. 2020 Dec 17;2020:9476749. doi: 10.1155/2020/9476749. eCollection 2020. J Ophthalmol. 2020. PMID: 33489350 Free PMC article.
-
Absent trochlear nerve with contralateral superior oblique underaction.Graefes Arch Clin Exp Ophthalmol. 2013 Sep;251(9):2297-8. doi: 10.1007/s00417-013-2355-y. Epub 2013 Apr 28. Graefes Arch Clin Exp Ophthalmol. 2013. PMID: 23624594 No abstract available.
References
-
- Holmes JM, Mutyala S, Maus TL, et al. . Pediatric third, fourth, and sixth nerve palsies: a population-based study. Am J Ophthalmol 1999;127:388–92 - PubMed
-
- Kim JH, Hwang JM. Magnetic resonance imaging in three patients with congenital oculomotor nerve palsy. Br J Ophthalmol 2009;93:1266–67 - PubMed
-
- Cheng YS, Zhou ZR, Peng WJ, et al. . Three-dimensional-fast imaging employing steady-state acquisition and T2-weighted fast spin-echo magnetic resonance sequences on visualization of cranial nerves III - XII. Chin Med J (Engl) 2008;121:276–79 - PubMed
-
- Fischbach F, Müller M, Bruhn H. High-resolution depiction of the cranial nerves in the posterior fossa (N III-N XII) with 2D fast spin echo and 3D gradient echo sequences at 3.0 T. Clin Imaging 2009;33:169–74 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical