

Steroid-resistant lymphatic remodeling in chronically inflamed mouse airways
- PMID: 20093490
- PMCID: PMC2832171
- DOI: 10.2353/ajpath.2010.090909
Steroid-resistant lymphatic remodeling in chronically inflamed mouse airways
Abstract
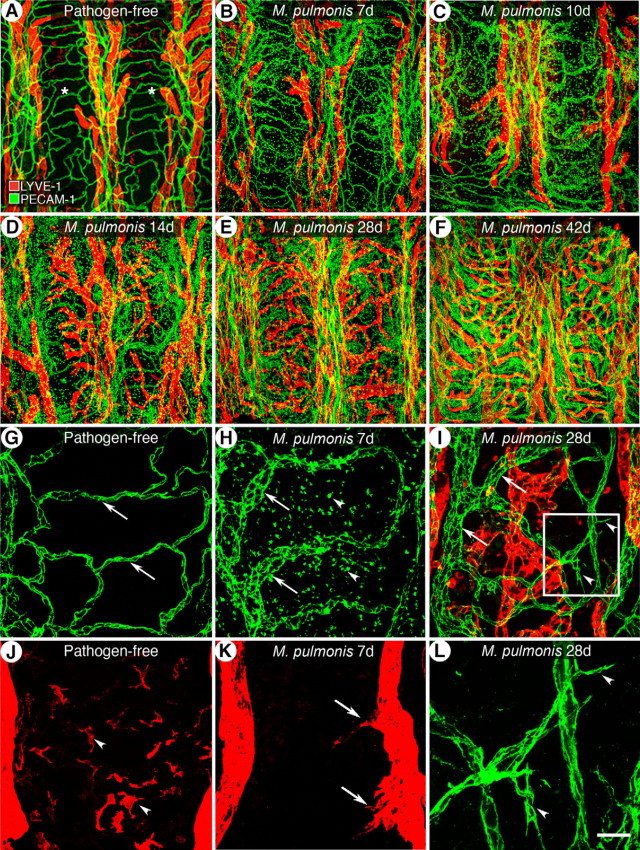
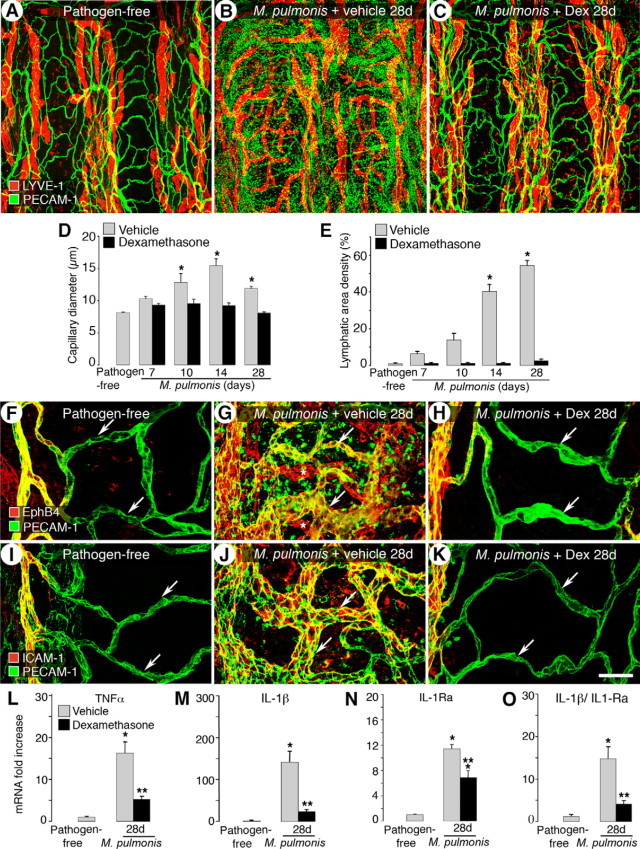
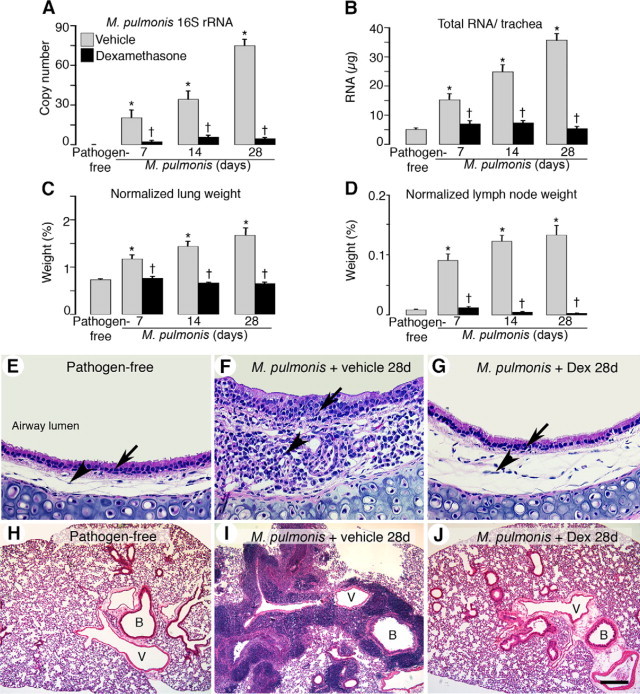
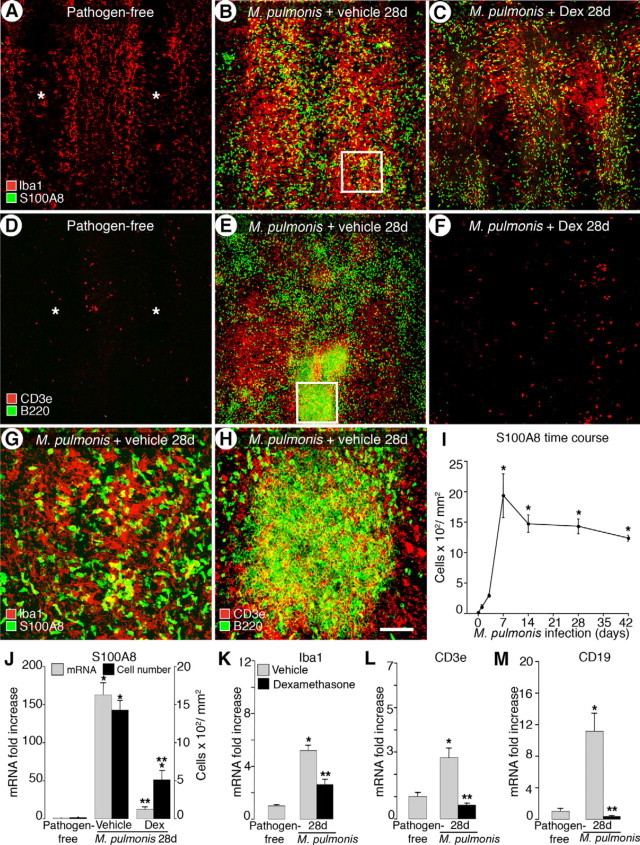
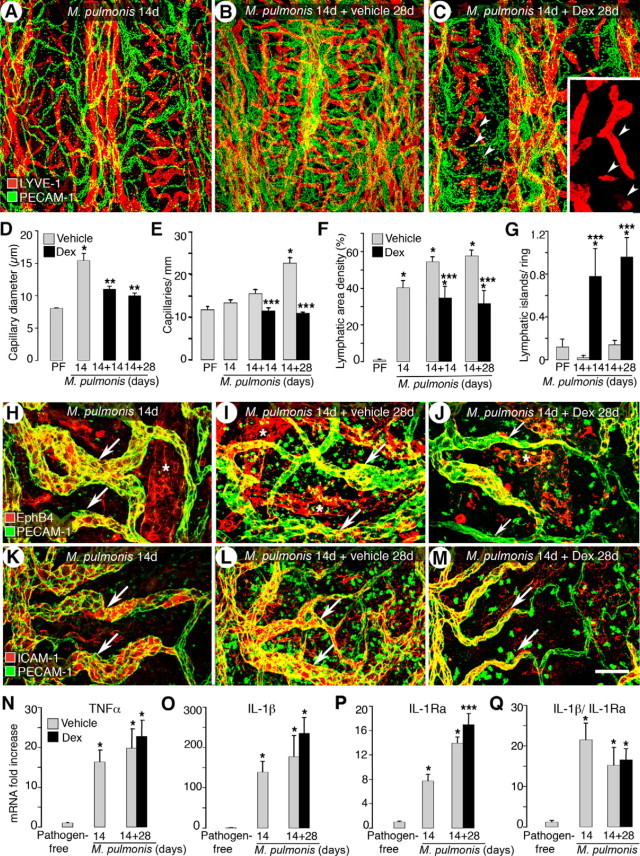
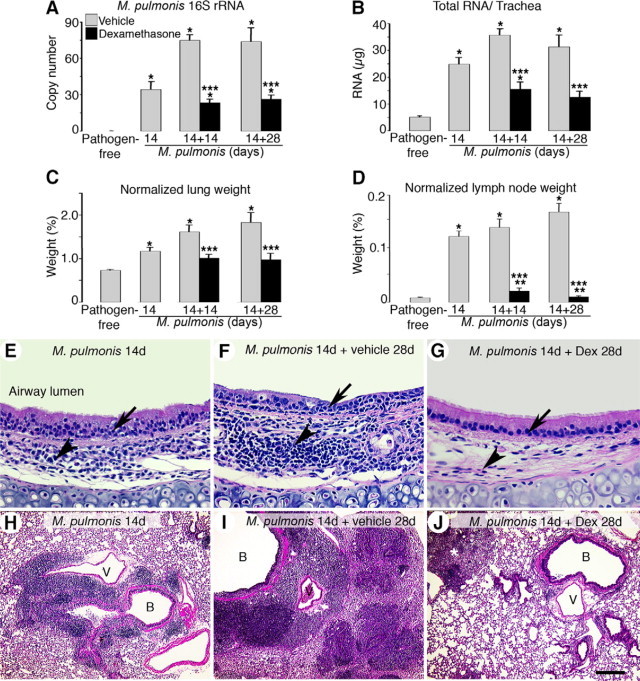
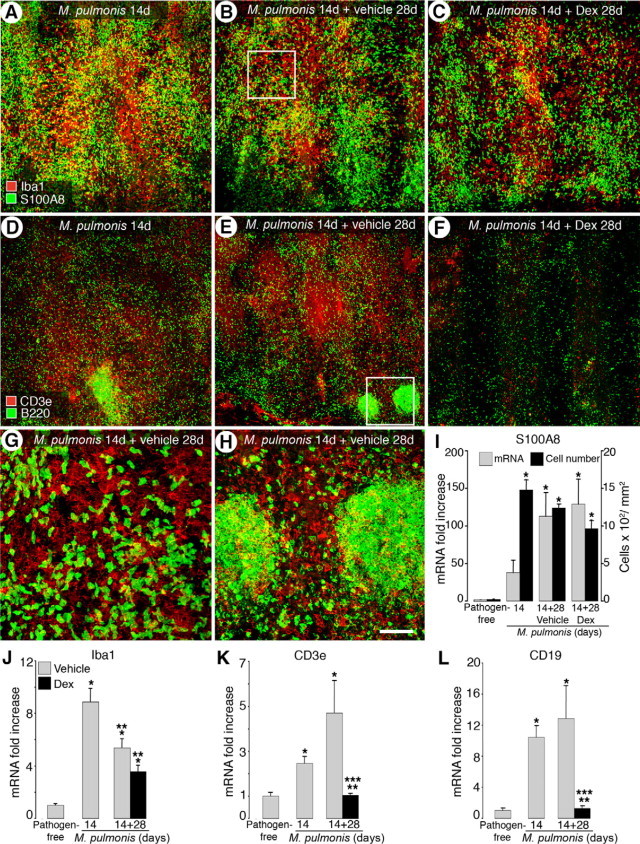
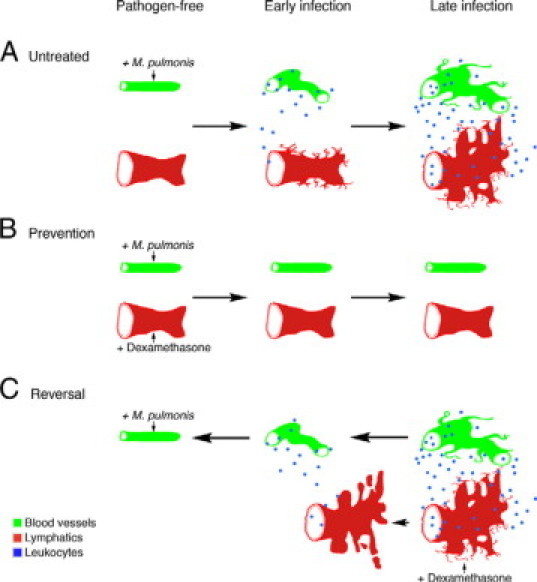
Angiogenesis and lymphangiogenesis participate in many inflammatory diseases, and their reversal is thought to be beneficial. However, the extent of reversibility of vessel remodeling is poorly understood. We exploited the potent anti-inflammatory effects of the corticosteroid dexamethasone to test the preventability and reversibility of vessel remodeling in Mycoplasma pulmonis-infected mice using immunohistochemistry and quantitative RT-PCR. In this model robust immune responses drive rapid and sustained changes in blood vessels and lymphatics. In infected mice not treated with dexamethasone, capillaries enlarged into venules expressing leukocyte adhesion molecules, sprouting angiogenesis and lymphangiogenesis occurred, and the inflammatory cytokines tumor necrosis factor and interleukin-1 increased. Concurrent dexamethasone treatment largely prevented the remodeling of blood vessels and lymphatics. Dexamethasone also significantly reduced cytokine expression, bacterial burden, and leukocyte influx into airways and lungs over 4 weeks of infection. In contrast, when infection was allowed to proceed untreated for 2 weeks and then was treated with dexamethasone for 4 weeks, most blood vessel changes reversed but lymphangiogenesis did not, suggesting that different survival mechanisms apply. Furthermore, dexamethasone significantly reduced the bacterial burden and influx of lymphocytes but not of neutrophils or macrophages or cytokine expression. These findings show that lymphatic remodeling is more resistant than blood vessel remodeling to corticosteroid-induced reversal. We suggest that lymphatic remodeling that persists after the initial inflammatory response has resolved may influence subsequent inflammatory episodes in clinical situations.
Figures
Similar articles
-
TNF-alpha drives remodeling of blood vessels and lymphatics in sustained airway inflammation in mice.J Clin Invest. 2009 Oct;119(10):2954-64. doi: 10.1172/JCI37626. Epub 2009 Sep 14. J Clin Invest. 2009. PMID: 19759514 Free PMC article.
-
alpha5beta1 Integrin blockade inhibits lymphangiogenesis in airway inflammation.Am J Pathol. 2009 Jun;174(6):2378-87. doi: 10.2353/ajpath.2009.080942. Epub 2009 May 14. Am J Pathol. 2009. PMID: 19443705 Free PMC article.
-
Synergistic actions of blocking angiopoietin-2 and tumor necrosis factor-α in suppressing remodeling of blood vessels and lymphatics in airway inflammation.Am J Pathol. 2015 Nov;185(11):2949-68. doi: 10.1016/j.ajpath.2015.07.010. Epub 2015 Sep 5. Am J Pathol. 2015. PMID: 26348576 Free PMC article.
-
Dynamics of airway blood vessels and lymphatics: lessons from development and inflammation.Proc Am Thorac Soc. 2011 Nov;8(6):504-7. doi: 10.1513/pats.201102-022MW. Proc Am Thorac Soc. 2011. PMID: 22052927 Free PMC article. Review.
-
Plasticity of airway lymphatics in development and disease.Adv Anat Embryol Cell Biol. 2014;214:41-54. doi: 10.1007/978-3-7091-1646-3_4. Adv Anat Embryol Cell Biol. 2014. PMID: 24276885 Free PMC article. Review.
Cited by
-
Visualization of intrapulmonary lymph vessels in healthy and inflamed murine lung using CD90/Thy-1 as a marker.PLoS One. 2013;8(2):e55201. doi: 10.1371/journal.pone.0055201. Epub 2013 Feb 8. PLoS One. 2013. PMID: 23408960 Free PMC article.
-
Physiological Perspective on Therapies of Lymphatic Vessels.Adv Wound Care (New Rochelle). 2018 Jul 1;7(7):189-208. doi: 10.1089/wound.2017.0768. Adv Wound Care (New Rochelle). 2018. PMID: 29984111 Free PMC article. Review.
-
Buttons and Zippers: Endothelial Junctions in Lymphatic Vessels.Cold Spring Harb Perspect Med. 2022 Dec 1;12(12):a041178. doi: 10.1101/cshperspect.a041178. Cold Spring Harb Perspect Med. 2022. PMID: 35534209 Free PMC article. Review.
-
The role of non-hematopoietic stromal cells in the persistence of inflammation.Front Immunol. 2013 Jan 14;3:416. doi: 10.3389/fimmu.2012.00416. eCollection 2012. Front Immunol. 2013. PMID: 23335923 Free PMC article.
-
Infection-induced lymphatic zippering restricts fluid transport and viral dissemination from skin.J Exp Med. 2022 May 2;219(5):e20211830. doi: 10.1084/jem.20211830. Epub 2022 Mar 30. J Exp Med. 2022. PMID: 35353138 Free PMC article.
References
-
- Halin C, Detmar M. Chapter 1. Inflammation, angiogenesis, and lymphangiogenesis. Methods Enzymol. 2008;445:1–25. - PubMed
-
- Jackson JR, Seed MP, Kircher CH, Willoughby DA, Winkler JD. The codependence of angiogenesis and chronic inflammation. FASEB J. 1997;11:457–465. - PubMed
-
- Walters EH, Reid D, Soltani A, Ward C. Angiogenesis: a potentially critical part of remodelling in chronic airway diseases? Pharmacol Ther. 2008;118:128–137. - PubMed
-
- Paredi P, Barnes PJ. The airway vasculature: recent advances and clinical implications. Thorax. 2009;64:444–450. - PubMed
-
- Van Kruiningen HJ, Colombel JF. The forgotten role of lymphangitis in Crohn's disease. Gut. 2008;57:1–4. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
