

Long-term dental visiting patterns and adult oral health
- PMID: 20093674
- PMCID: PMC2821461
- DOI: 10.1177/0022034509356779
Long-term dental visiting patterns and adult oral health
Abstract
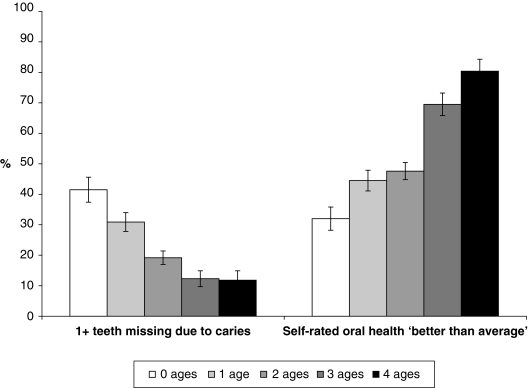
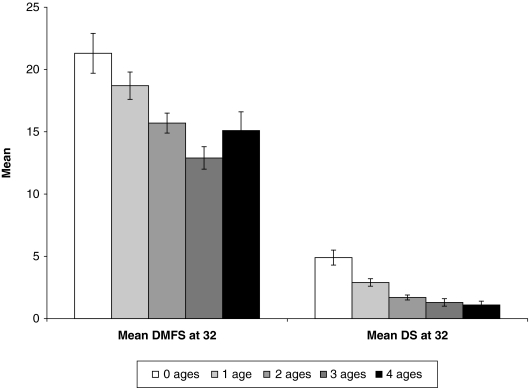
To date, the evidence supporting the benefits of dental visiting comes from cross-sectional studies. We investigated whether long-term routine dental visiting was associated with lower experience of dental caries and missing teeth, and better self-rated oral health, by age 32. A prospective cohort study in New Zealand examined 932 participants' use of dentistry at ages 15, 18, 26, and 32. At each age, routine attenders (RAs) were identified as those who (a) usually visited for a check-up, and (b) had made a dental visit during the previous 12 months. Routine attending prevalence fell from 82% at age 15 to 28% by 32. At any given age, routine attenders had better-than-average oral health, fewer had teeth missing due to caries, and they had lower mean DS and DMFS scores. By age 32, routine attenders had better self-reported oral health and less tooth loss and caries. The longer routine attendance was maintained, the stronger the effect. Routine dental attendance is associated with better oral health.
Figures
References
-
- Axelsson P, Lindhe J, Nyström B. (1991). On the prevention of caries andperiodontal disease: results of a 15-year longitudinal study in adults. J Clin Periodontol 18:182-189 - PubMed
-
- Baelum V. (2008). Caries management: technical solutions to biological problems or evidence-based care? J Oral Rehabil 35:135-151 - PubMed
-
- Davenport CF, Elley KM, Fry-Smith A, Taylor-Weetman CL, Taylor RS. (2003). The effectiveness of routine dental checks: a systematic review of the evidence base. Br Dent J 195:87-98 - PubMed
-
- Dixon GS, Thomson WM, Kruger E. (1999). The West Coast Study I: self-reported dental health and use of dental services. NZ Dent J 95:38-43 - PubMed
-
- Elley WB, Irving JC. (1985). The Elley-Irving socio-economic index 1981 Census revision. NZ J Educ Stud 20:115-128
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
