

Barrett's oesophagus and oesophageal adenocarcinoma: time for a new synthesis
- PMID: 20094044
- PMCID: PMC2879265
- DOI: 10.1038/nrc2773
Barrett's oesophagus and oesophageal adenocarcinoma: time for a new synthesis
Abstract
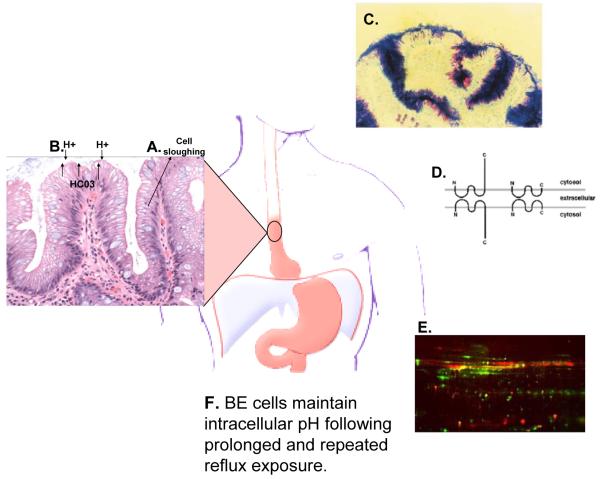
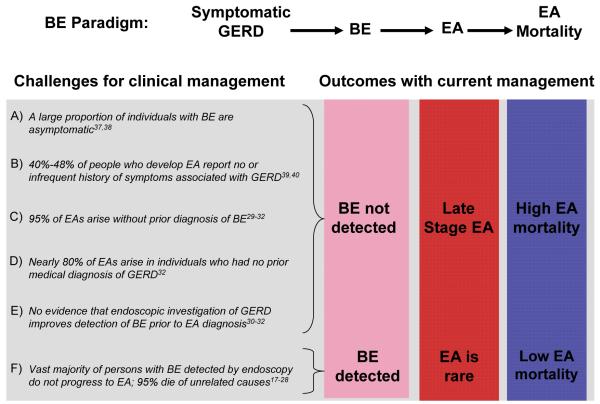
The public health importance of Barrett's oesophagus lies in its association with oesophageal adenocarcinoma. The incidence of oesophageal adenocarcinoma has risen at an alarming rate over the past four decades in many regions of the Western world, and there are indications that the incidence of this disease is on the rise in Asian populations in which it has been rare. Much has been learned of host and environmental risk factors that affect the incidence of oesophageal adenocarcinoma, and data indicate that patients with Barrett's oesophagus rarely develop oesophageal adenocarcinoma. Given that 95% of oesophageal adenocarcinomas arise in individuals without a prior diagnosis of Barrett's oesophagus, what strategies can be used to reduce late diagnosis of oesophageal adenocarcinoma?
Figures
References
-
- Sharma P, et al. A critical review of the diagnosis and management of Barrett’s esophagus: the AGA Chicago Workshop. Gastroenterology. 2004;127:310–30. - PubMed
-
- Vakil N, van Zanten SV, Kahrilas P, Dent J, Jones R. The Montreal definition and classification of gastroesophageal reflux disease: a global evidence-based consensus. Am J Gastroenterol. 2006;101:1900–20. quiz 1943. - PubMed
-
- Barrett N. Chronic peptic ulcer of the oesophagus and ‘oesophagitis’. Br J Surg. 1950;38:175–182. - PubMed
-
- Naef AP, Savary M, Ozzello L. Columnar-lined lower esophagus: an acquired lesion with malignant predisposition. Report on 140 cases of Barrett’s esophagus with 12 adenocarcinomas. Journal of Thoracic and Cardiovascular Surgery. 1975;70:826–35. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
