

Reducing radiation dose to selected organs by selecting the tube start angle in MDCT helical scans: a Monte Carlo based study
- PMID: 20095278
- PMCID: PMC2797045
- DOI: 10.1118/1.3259773
Reducing radiation dose to selected organs by selecting the tube start angle in MDCT helical scans: a Monte Carlo based study
Abstract
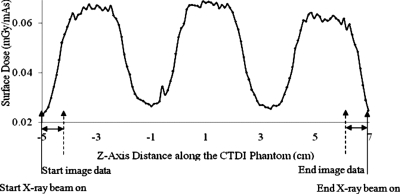
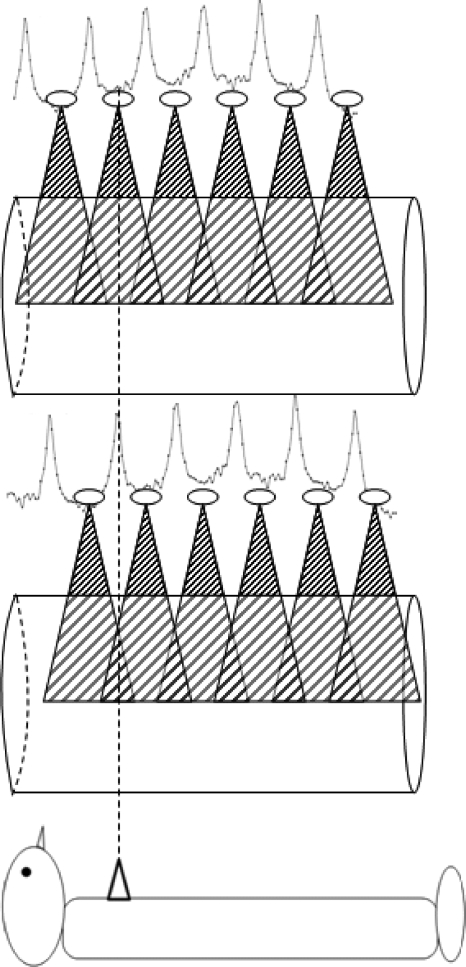
Purpose: Previous work has demonstrated that there are significant dose variations with a sinusoidal pattern on the peripheral of a CTDI 32 cm phantom or on the surface of an anthropomorphic phantom when helical CT scanning is performed, resulting in the creation of "hot" spots or "cold" spots. The purpose of this work was to perform preliminary investigations into the feasibility of exploiting these variations to reduce dose to selected radiosensitive organs solely by varying the tube start angle in CT scans.
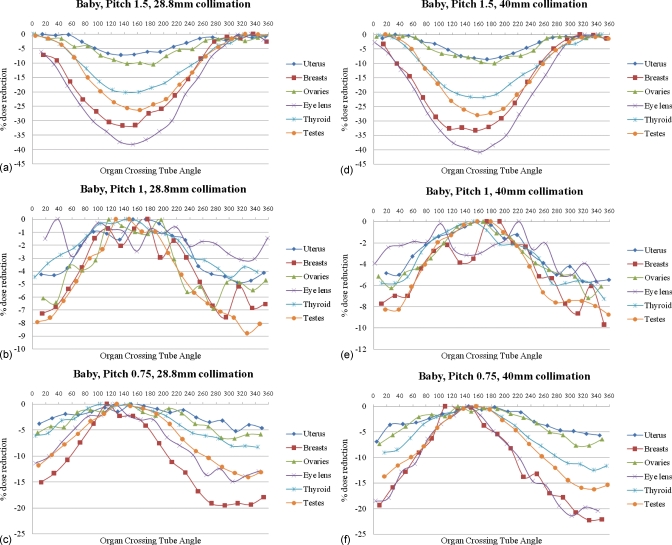
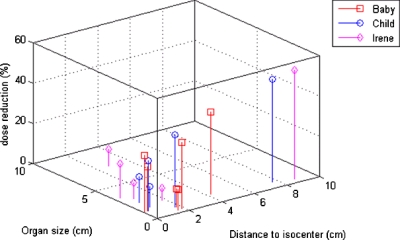
Methods: Radiation dose to several radiosensitive organs (including breasts, thyroid, uterus, gonads, and eye lenses) resulting from MDCT scans were estimated using Monte Carlo simulation methods on voxelized patient models, including GSF's Baby, Child, and Irene. Dose to fetus was also estimated using four pregnant female models based on CT images of the pregnant patients. Whole-body scans were simulated using 120 kVp, 300 mAs, both 28.8 and 40 mm nominal collimations, and pitch values of 1.5, 1.0, and 0.75 under a wide range of start angles (0 degree-340 degrees in 20 degrees increments). The relationship between tube start angle and organ dose was examined for each organ, and the potential dose reduction was calculated.
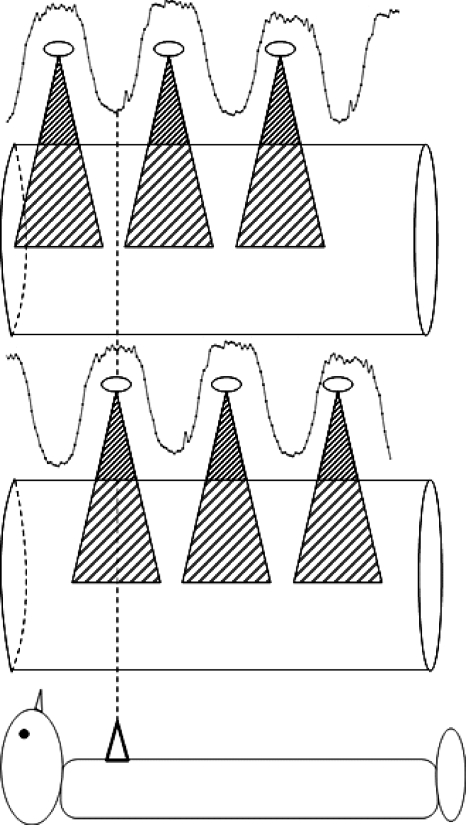
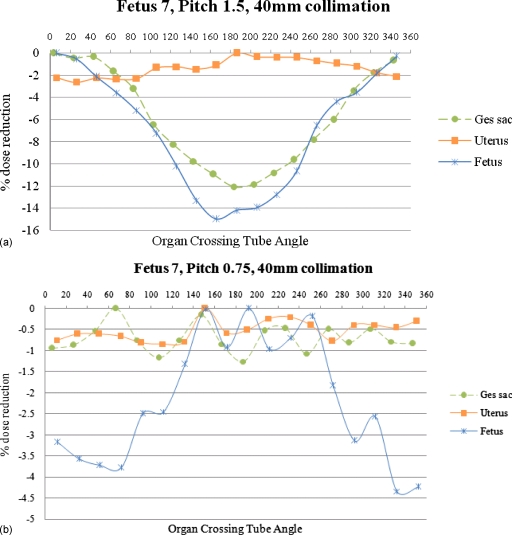
Results: Some organs exhibit a strong dose variation, depending on the tube start angle. For small peripheral organs (e.g., the eye lenses of the Baby phantom at pitch 1.5 with 40 mm collimation), the minimum dose can be 41% lower than the maximum dose, depending on the tube start angle. In general, larger dose reductions occur for smaller peripheral organs in smaller patients when wider collimation is used. Pitch 1.5 and pitch 0.75 have different mechanisms of dose reduction. For pitch 1.5 scans, the dose is usually lowest when the tube start angle is such that the x-ray tube is posterior to the patient when it passes the longitudinal location of the organ. For pitch 0.75 scans, the dose is lowest when the tube start angle is such that the x-ray tube is anterior to the patient when it passes the longitudinal location of the organ.
Conclusions: Helical MDCT scanning at pitch 1.5 and pitch 0.75 results in "cold spots" and "hot spots" that are created both at surface and in-depth locations within patients. For organs that have a relatively small longitudinal extent, dose can vary considerably with different start angles. While current MDCT systems do not provide the user with the ability to control the tube start angle, these results indicate that in these specific situations (pitch 1.5 or pitch 0.75, small organs and especially small patients), there could be significant dose savings to organs if that functionality would be provided.
Figures
Similar articles
-
Variability of surface and center position radiation dose in MDCT: Monte Carlo simulations using CTDI and anthropomorphic phantoms.Med Phys. 2009 Mar;36(3):1025-38. doi: 10.1118/1.3078053. Med Phys. 2009. PMID: 19378763 Free PMC article.
-
Organ dose and inherent uncertainty in helical CT dosimetry due to quasiperiodic dose distributions.Med Phys. 2011 Jun;38(6):3177-85. doi: 10.1118/1.3590367. Med Phys. 2011. PMID: 21815392
-
A Monte Carlo based method to estimate radiation dose from multidetector CT (MDCT): cylindrical and anthropomorphic phantoms.Phys Med Biol. 2005 Sep 7;50(17):3989-4004. doi: 10.1088/0031-9155/50/17/005. Epub 2005 Aug 11. Phys Med Biol. 2005. PMID: 16177525
-
Patient radiation risk reduction by controlling the tube start angle in single and dual source spiral CT scans: A simulation study.Med Phys. 2024 Oct;51(10):7080-7092. doi: 10.1002/mp.17290. Epub 2024 Jul 11. Med Phys. 2024. PMID: 38991121
-
Estimating radiation doses from multidetector CT using Monte Carlo simulations: effects of different size voxelized patient models on magnitudes of organ and effective dose.Phys Med Biol. 2007 May 7;52(9):2583-97. doi: 10.1088/0031-9155/52/9/017. Epub 2007 Apr 17. Phys Med Biol. 2007. PMID: 17440254
Cited by
-
A comparison of methods to estimate organ doses in CT when utilizing approximations to the tube current modulation function.Med Phys. 2012 Aug;39(8):5212-28. doi: 10.1118/1.4736807. Med Phys. 2012. PMID: 22894446 Free PMC article.
-
A fast, linear Boltzmann transport equation solver for computed tomography dose calculation (Acuros CTD).Med Phys. 2019 Feb;46(2):925-933. doi: 10.1002/mp.13305. Epub 2018 Dec 24. Med Phys. 2019. PMID: 30471131 Free PMC article.
-
Patient-specific radiation dose and cancer risk estimation in CT: part II. Application to patients.Med Phys. 2011 Jan;38(1):408-19. doi: 10.1118/1.3515864. Med Phys. 2011. PMID: 21361209 Free PMC article.
-
A real-time Monte Carlo tool for individualized dose estimations in clinical CT.Phys Med Biol. 2019 Nov 4;64(21):215020. doi: 10.1088/1361-6560/ab467f. Phys Med Biol. 2019. PMID: 31539892 Free PMC article.
-
Patient-specific radiation dose and cancer risk estimation in CT: part I. development and validation of a Monte Carlo program.Med Phys. 2011 Jan;38(1):397-407. doi: 10.1118/1.3515839. Med Phys. 2011. PMID: 21361208 Free PMC article.
References
-
- NCRP, “Ionizing radiation exposure of the population of the United States,” NCRP Report No. 160, 2009. - PubMed
-
- Udayasankar U. K., Braithwaite K., Arvaniti M., Tudorascu D., Small W. C., Little S., and Palasis S., “Low-dose nonenhanced head CT protocol for follow-up evaluation of children with ventriculoperitoneal shunt: Reduction of radiation and effect on image quality,” AJNR Am. J. Neuroradiol. ZZZZZZ 29, 802–806 (2008).10.3174/ajnr.A0923 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
