

Hypocitraturia and hyperoxaluria after Roux-en-Y gastric bypass surgery
- PMID: 20096421
- PMCID: PMC3293469
- DOI: 10.1016/j.juro.2009.11.022
Hypocitraturia and hyperoxaluria after Roux-en-Y gastric bypass surgery
Abstract
Purpose: Roux-en-Y gastric bypass surgery is associated with an increased risk of nephrolithiasis but obesity itself is a known risk factor for kidney stones. To assess the mechanism(s) predisposing to nephrolithiasis after Roux-en-Y gastric bypass we compared urinary tract stone risk profiles in patients who underwent the procedure and normal obese individuals.
Materials and methods: In this cross-sectional study urine and serum biochemistry was evaluated in 19 nonstone forming patients after Roux-en-Y gastric bypass and in 19 gender, age and body mass index matched obese controls without a history of nephrolithiasis.
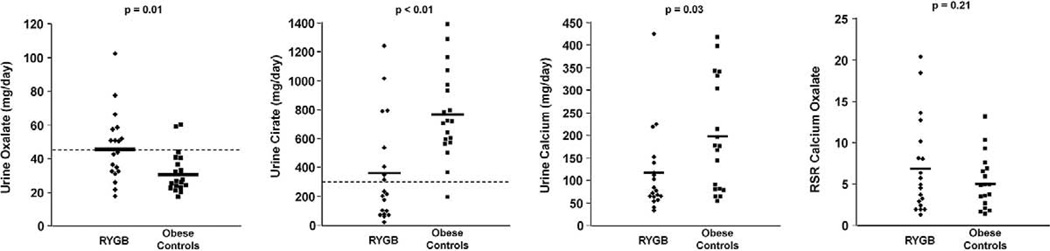
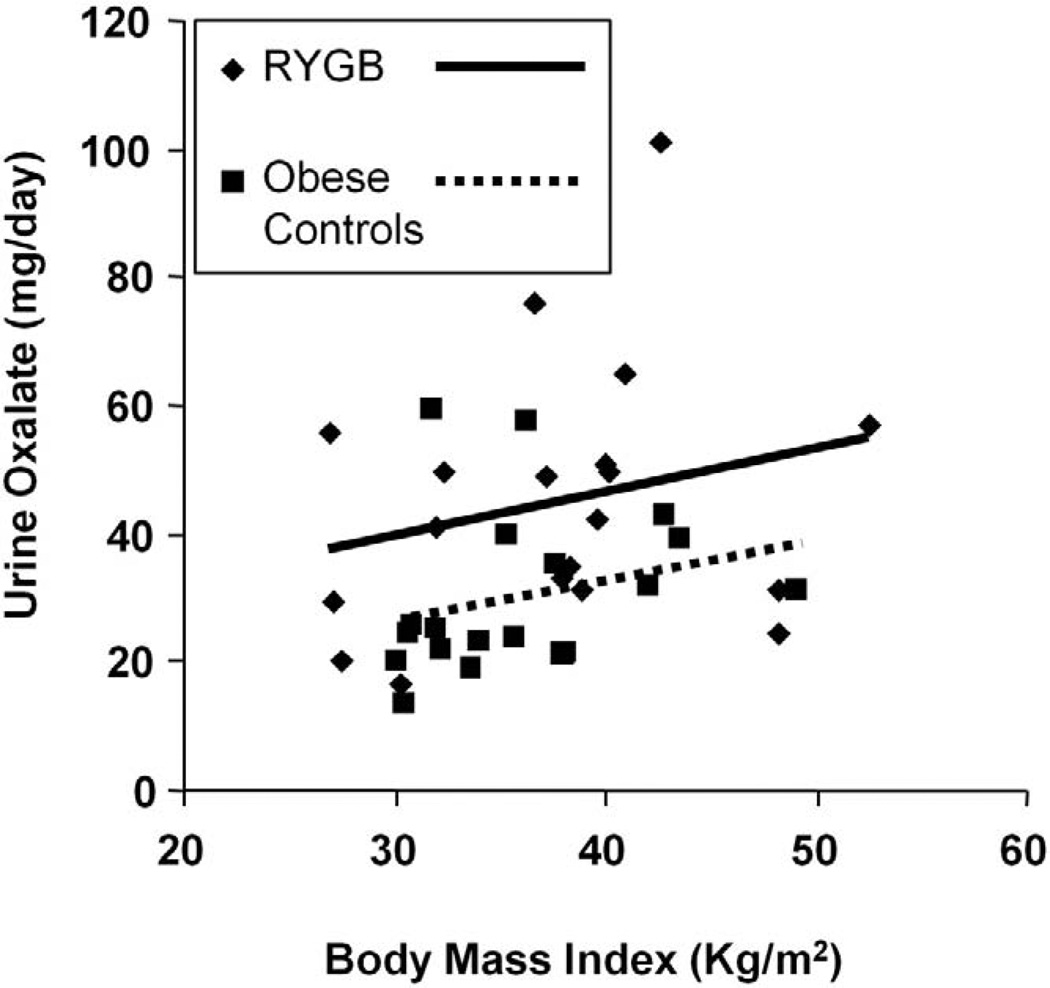
Results: Compared with obese controls surgical patients had significantly higher mean +/- SD urine oxalate (45 +/- 21 vs 30 +/- 11 mg daily, p = 0.01) and lower urine citrate (358 +/- 357 vs 767 +/- 307 mg daily, p <0.01). The prevalence of hyperoxaluria (47% vs 10.5%, p = 0.02) and hypocitraturia (63% vs 5%, p <0.01) was significantly higher in surgical patients, who also had significantly lower urine calcium than obese controls (115 +/- 93 vs 196 +/- 123 mg daily, p = 0.03). The calcium oxalate urine relative supersaturation ratio was not significantly different between the 2 groups.
Conclusions: Almost half of patients with Roux-en-Y gastric bypass without a history of nephrolithiasis showed hyperoxaluria or hypocitraturia. This prevalence was significantly higher than in body mass index matched controls. These risk factors were negated by lower urine calcium excretion in patients with Roux-en-Y gastric bypass.
2010 American Urological Association Education and Research, Inc. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Santry HP, Gillen DL, Lauderdale DS. Trends in bariatric surgical procedures. JAMA. 2005;294:1909. - PubMed
-
- Kirkpatrick JR. Jejunoileal bypass. A legacy of late complications. Arch Surg. 1987;122:610. - PubMed
-
- Requarth JA, Burchard KW, Colacchio TA, et al. Long-term morbidity following jejunoileal bypass. The continuing potential need for surgical reversal. Arch Surg. 1995;130:318. - PubMed
-
- Asplin JR, Coe FL. Hyperoxaluria in kidney stone formers treated with modern bariatric surgery. J Urol. 2007;177:565. - PubMed
-
- Nelson WK, Houghton SG, Milliner DS, et al. Enteric hyperoxaluria, nephrolithiasis, and oxalate nephropathy: potentially serious and unappreciated complications of Roux-en-Y gastric bypass. Surg Obes Relat Dis. 2005;1:481. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
