

{beta}-Cell secretory capacity and demand in recipients of islet, pancreas, and kidney transplants
- PMID: 20097708
- PMCID: PMC2841536
- DOI: 10.1210/jc.2009-2289
{beta}-Cell secretory capacity and demand in recipients of islet, pancreas, and kidney transplants
Abstract
Context: beta-Cell secretory capacity, a measure of functional beta-cell mass, is often impaired in islet transplant recipients, likely because of a low engrafted beta-cell mass, although calcineurin inhibitor toxicity is often cited as the explanation.
Objective: We sought to determine whether use of the calcineurin inhibitor tacrolimus was associated with reduced beta-cell secretory capacity or with increased beta-cell secretory demand independent of engrafted islet mass.
Design and participants: We compared metabolic measures in five intraportal islet recipients vs. 10 normal controls and in seven portally-drained pancreas-kidney and eight nondiabetic kidney recipients vs. nine kidney donor controls. All transplant groups received comparable exposure to tacrolimus, and each transplant group was matched for kidney function to its respective control group.
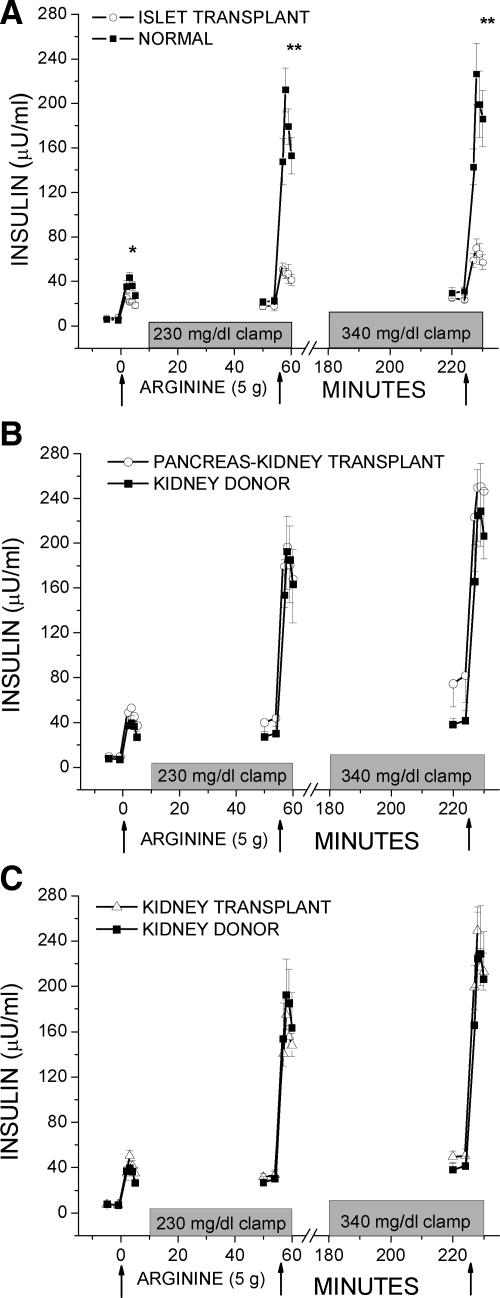
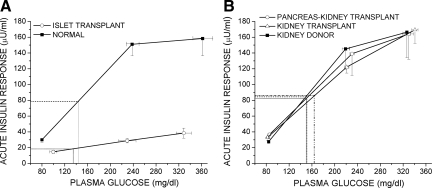
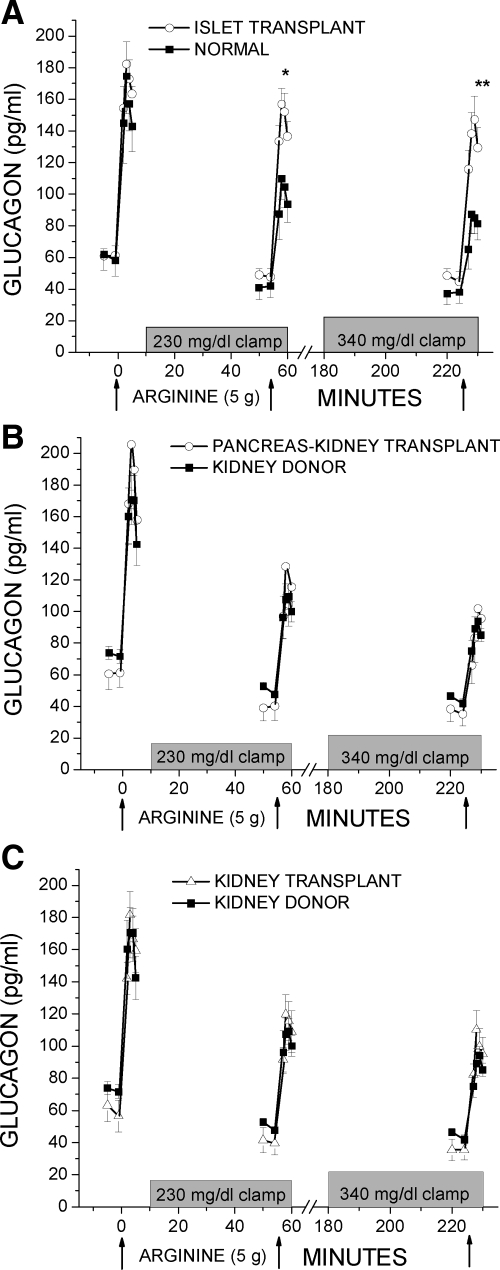
Intervention and main outcome measures: All participants underwent glucose-potentiated arginine testing where acute insulin responses to arginine (5 g) were determined under fasting (AIR(arg)), 230 mg/dl (AIR(pot)), and 340 mg/dl (AIR(max)) clamp conditions, and AIR(max) gives the beta-cell secretory capacity. Insulin sensitivity (M/I) and proinsulin secretory ratios (PISRs) were assessed to determine whether tacrolimus increased beta-cell secretory demand.
Results: Insulin responses were significantly lower than normal in the islet group for AIR(arg) (P < 0.05), AIR(pot) (P < 0.01), and AIR(max) (P < 0.01), whereas responses in the pancreas-kidney and kidney transplant groups were not different than in the kidney donor group. M/I and PISRs were not different in any of the transplant vs. control groups.
Conclusions: Impaired beta-cell secretory capacity in islet transplantation is best explained by a low engrafted beta-cell mass and not by a deleterious effect of tacrolimus.
Figures
References
-
- Shapiro AM, Ricordi C, Hering BJ, Auchincloss H, Lindblad R, Robertson RP, Secchi A, Brendel MD, Berney T, Brennan DC, Cagliero E, Alejandro R, Ryan EA, DiMercurio B, Morel P, Polonsky KS, Reems JA, Bretzel RG, Bertuzzi F, Froud T, Kandaswamy R, Sutherland DE, Eisenbarth G, Segal M, Preiksaitis J, Korbutt GS, Barton FB, Viviano L, Seyfert-Margolis V, Bluestone J, Lakey JR 2006 International trial of the Edmonton protocol for islet transplantation. N Engl J Med 355:1318–1330 - PubMed
-
- Rickels MR, Schutta MH, Markmann JF, Barker CF, Naji A, Teff KL 2005 β-Cell function following human islet transplantation for type 1 diabetes. Diabetes 54:100–106 - PubMed
-
- Keymeulen B, Gillard P, Mathieu C, Movahedi B, Maleux G, Delvaux G, Ysebaert D, Roep B, Vandemeulebroucke E, Marichal M, In 't Veld P, Bogdani M, Hendrieckx C, Gorus F, Ling Z, van Rood J, Pipeleers D 2006 Correlation between β cell mass and glycemic control in type 1 diabetic recipients of islet cell graft. Proc Natl Acad Sci USA 103:17444–17449 - PMC - PubMed
-
- Kahn SE, Carr DB, Faulenbach MV, Utzschneider KM 2008 An examination of β-cell function measures and their potential use for estimating β-cell mass. Diabetes Obes Metab 10 (Suppl 4):63–76 - PubMed
-
- Eriksson O, Eich T, Sundin A, Tibell A, Tufveson G, Andersson H, Felldin M, Foss A, Kyllönen L, Langstrom B, Nilsson B, Korsgren O, Lundgren T 2009 Positron emission tomography in clinical islet transplantation. Am J Transplant 9:2816–2824 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
