

Sexual seroadaptation: lessons for prevention and sex research from a cohort of HIV-positive men who have sex with men
- PMID: 20098616
- PMCID: PMC2809110
- DOI: 10.1371/journal.pone.0008831
Sexual seroadaptation: lessons for prevention and sex research from a cohort of HIV-positive men who have sex with men
Abstract
Background: Surveillance data on sexually transmitted infections (STIs) and behavioral characteristics identified in studies of the risk of seroconversion are often used as to track sexual behaviors that spread HIV. However, such analyses can be confounded by "seroadaptation"--the restriction of unprotected anal intercourse (UAI), especially unprotected insertive UAI, to seroconcordant partnerships.
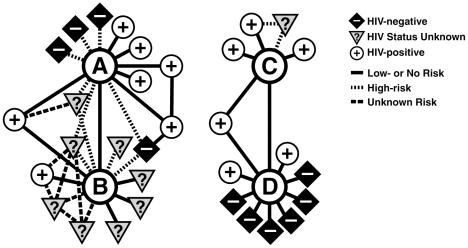
Methods: We utilized sexual network methodology and repeated-measures statistics to test the hypothesis that seroadaptive strategies reduce the risk of HIV transmission despite numerous partnerships and frequent UAI.
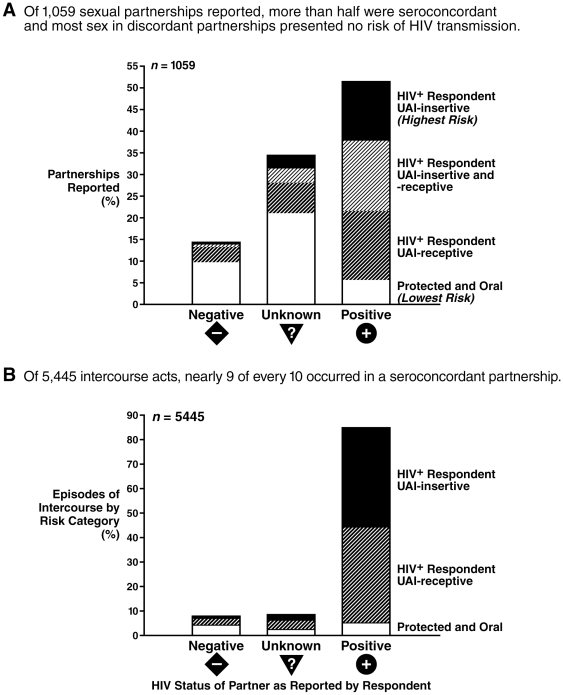
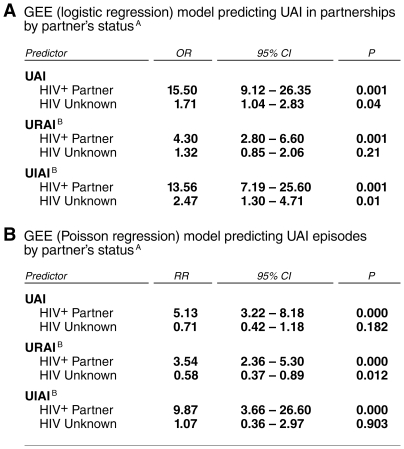
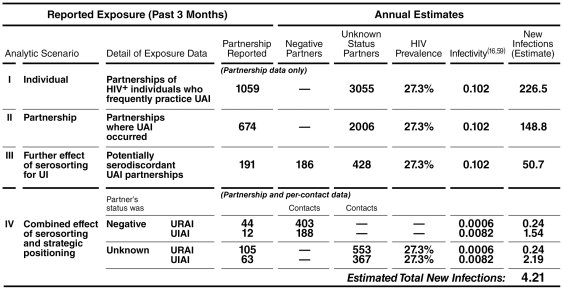
Principal findings: In a prospective cohort study of HIV superinfection including 168 HIV-positive men who have sex with men (MSM), we found extensive seroadaptation. UAI was 15.5 times more likely to occur with a positive partner than a negative one (95% confidence interval [CI], 9.1-26.4). Receptive UAI was 4.3 times more likely in seroconcordant partnerships than with negative partners (95% CI, 2.8-6.6), but insertive UAI was 13.6 times more likely with positives (95% CI, 7.2-25.6). Our estimates suggest that seroadaptation reduced HIV transmissions by 98%.
Conclusion: Potentially effective HIV prevention strategies, such as seroadaptation, have evolved in communities of MSM before they have been recognized in research or discussed in the public health forum. Thus, to be informative, studies of HIV risk must be designed to assess seroadaptive behaviors rather than be limited to individual characteristics, unprotected intercourse, and numbers of partners. STI surveillance is not an effective indicator of trends in HIV incidence where there are strong patterns of seroadaptation.
Conflict of interest statement
Figures
Similar articles
-
Seroadaptive practices: association with HIV acquisition among HIV-negative men who have sex with men.PLoS One. 2012;7(10):e45718. doi: 10.1371/journal.pone.0045718. Epub 2012 Oct 3. PLoS One. 2012. PMID: 23056215 Free PMC article.
-
Association between serosorting and bacterial sexually transmitted infection among HIV-negative men who have sex with men at an urban lesbian, gay, bisexual, and transgender health center.Sex Transm Dis. 2012 Dec;39(12):959-64. doi: 10.1097/OLQ.0b013e31826e870d. Sex Transm Dis. 2012. PMID: 23191950
-
Perceived HIV status is a key determinant of unprotected anal intercourse within partnerships of men who have sex with men in Amsterdam.AIDS Behav. 2014 Dec;18(12):2442-56. doi: 10.1007/s10461-014-0819-7. AIDS Behav. 2014. PMID: 24920343
-
Internet-based partner selection and risk for unprotected anal intercourse in sexual encounters among men who have sex with men: a meta-analysis of observational studies.Sex Transm Infect. 2014 Jun;90(4):290-6. doi: 10.1136/sextrans-2013-051332. Epub 2014 Feb 11. Sex Transm Infect. 2014. PMID: 24518249 Review.
-
Prevalence of unprotected anal intercourse among HIV-diagnosed MSM in the United States: a meta-analysis.AIDS. 2009 Aug 24;23(13):1617-29. doi: 10.1097/QAD.0b013e32832effae. AIDS. 2009. PMID: 19584704 Review.
Cited by
-
Social networks, sexual networks and HIV risk in men who have sex with men.Curr HIV/AIDS Rep. 2014 Mar;11(1):81-92. doi: 10.1007/s11904-013-0194-4. Curr HIV/AIDS Rep. 2014. PMID: 24384832 Free PMC article. Review.
-
The HIV Environmental Riskscape: The Roles of HIV Sexual Risk and Resilience Factors among Black Men Who Have Sex with Men: Findings from the Real Talk Project.AIDS Behav. 2024 Oct;28(10):3228-3237. doi: 10.1007/s10461-024-04418-8. Epub 2024 Jun 20. AIDS Behav. 2024. PMID: 38900312
-
Developing a conceptual framework of seroadaptive behaviors in HIV-diagnosed men who have sex with men.J Infect Dis. 2014 Dec 1;210 Suppl 2(Suppl 2):S586-93. doi: 10.1093/infdis/jiu482. J Infect Dis. 2014. PMID: 25381379 Free PMC article. Review.
-
Changes in seroadaptive practices from before to after diagnosis of recent HIV infection among men who have sex with men.PLoS One. 2013;8(2):e55397. doi: 10.1371/journal.pone.0055397. Epub 2013 Feb 6. PLoS One. 2013. PMID: 23405145 Free PMC article.
-
Factors associated with unprotected anal sex with multiple non-steady partners in the past 12 months: results from the European Men-Who-Have-Sex-With-Men Internet Survey (EMIS 2010).BMC Public Health. 2016 Jan 19;16:47. doi: 10.1186/s12889-016-2691-z. BMC Public Health. 2016. PMID: 26781647 Free PMC article.
References
-
- Fox KK, Whittington WL, Levine WC, Moran JS, Zaidi AA, et al. Gonorrhea in the United States, 1981-1996. Demographic and geographic trends. Sex Transm Dis. 1998;25:386–393. - PubMed
-
- Ekstrand ML, Stall RD, Paul JP, Osmond DH, Coates TJ. Gay men report high rates of unprotected anal sex with partners of unknown or discordant HIV status. Aids. 1999;13:1525–1533. - PubMed
