

The relationship between anti-merozoite antibodies and incidence of Plasmodium falciparum malaria: A systematic review and meta-analysis
- PMID: 20098724
- PMCID: PMC2808214
- DOI: 10.1371/journal.pmed.1000218
The relationship between anti-merozoite antibodies and incidence of Plasmodium falciparum malaria: A systematic review and meta-analysis
Abstract
Background: One of the criteria to objectively prioritize merozoite antigens for malaria vaccine development is the demonstration that naturally acquired antibodies are associated with protection from malaria. However, published evidence of the protective effect of these antibodies is conflicting.
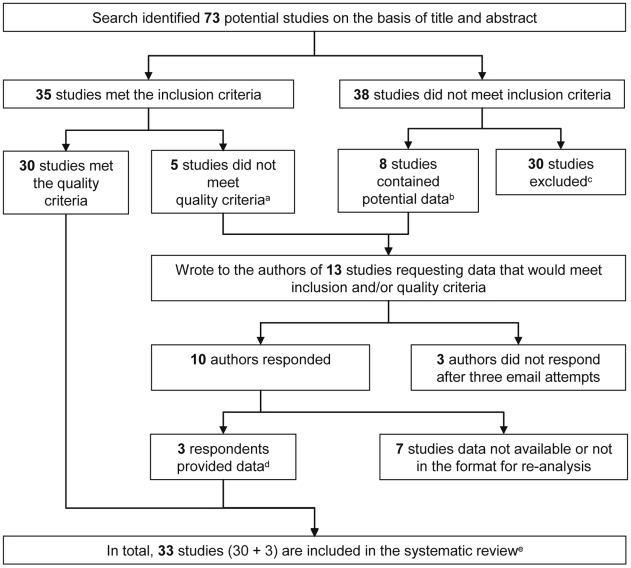
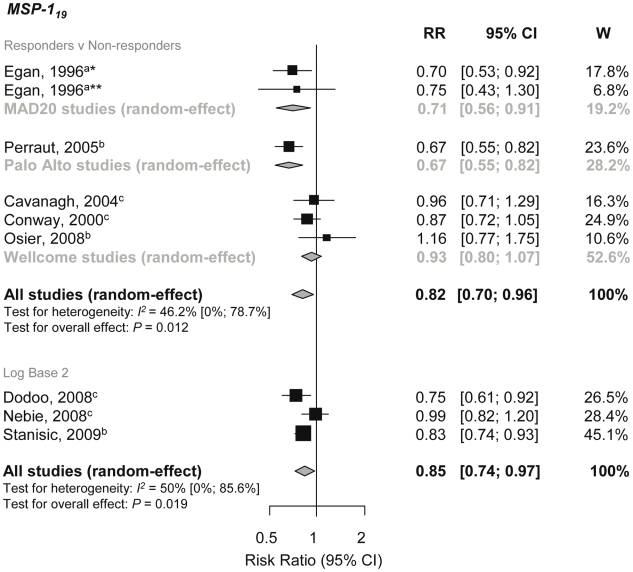
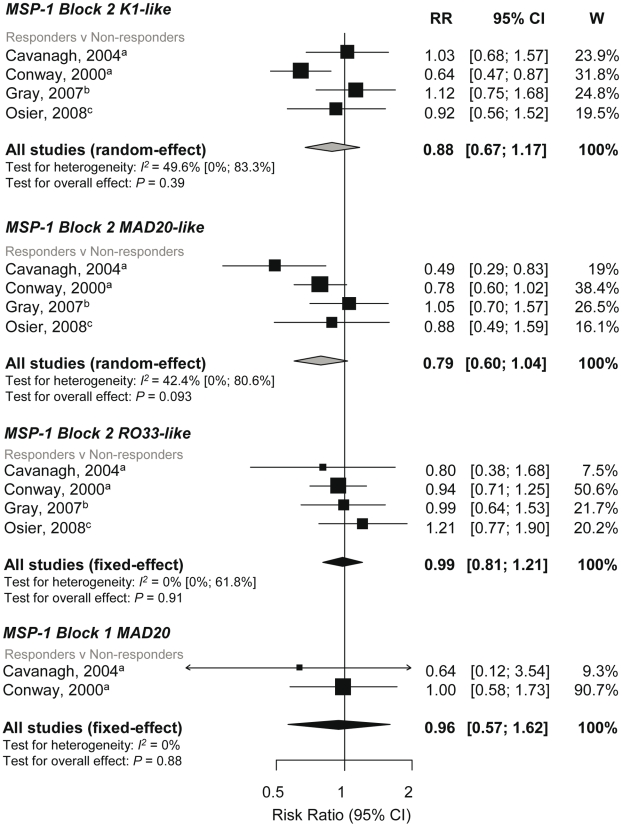
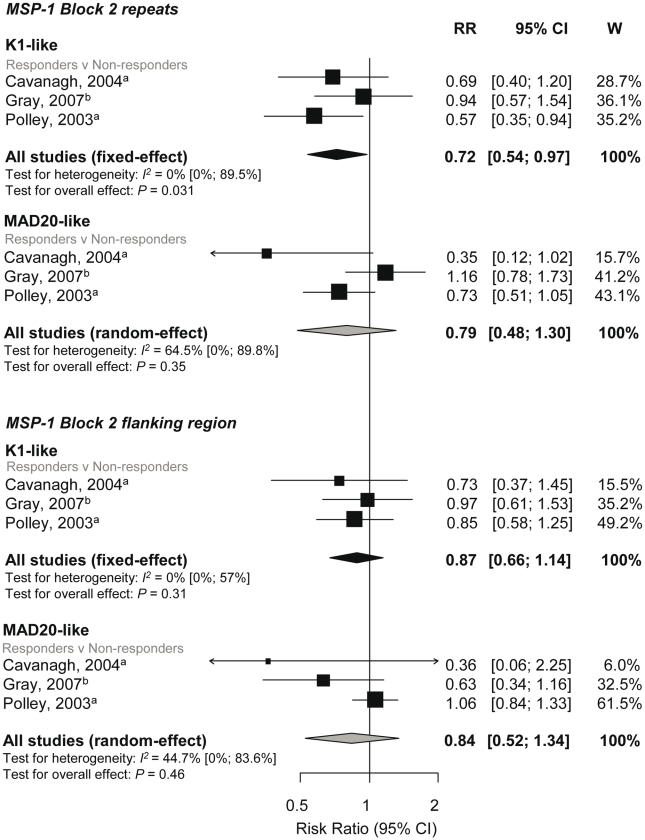
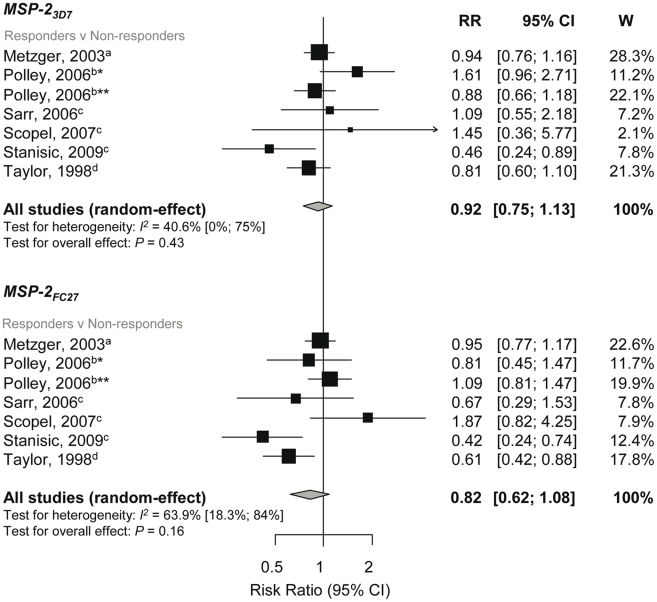
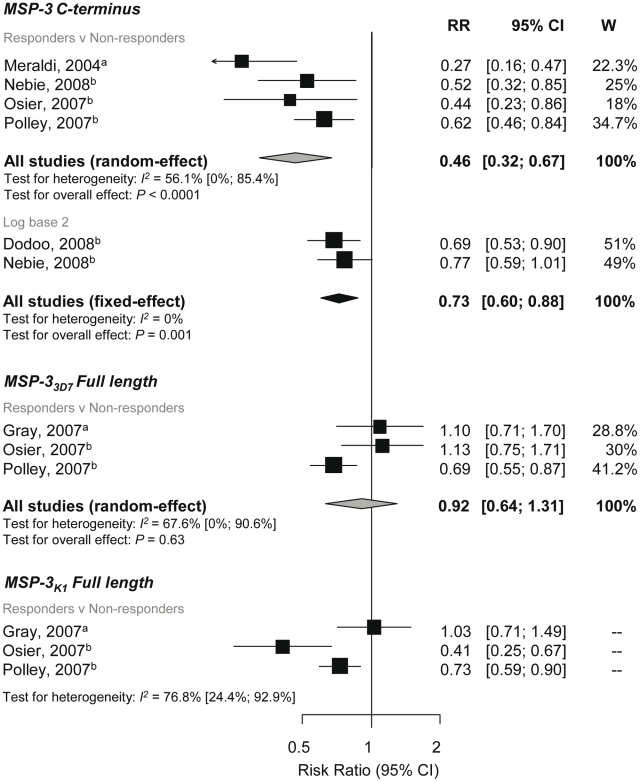
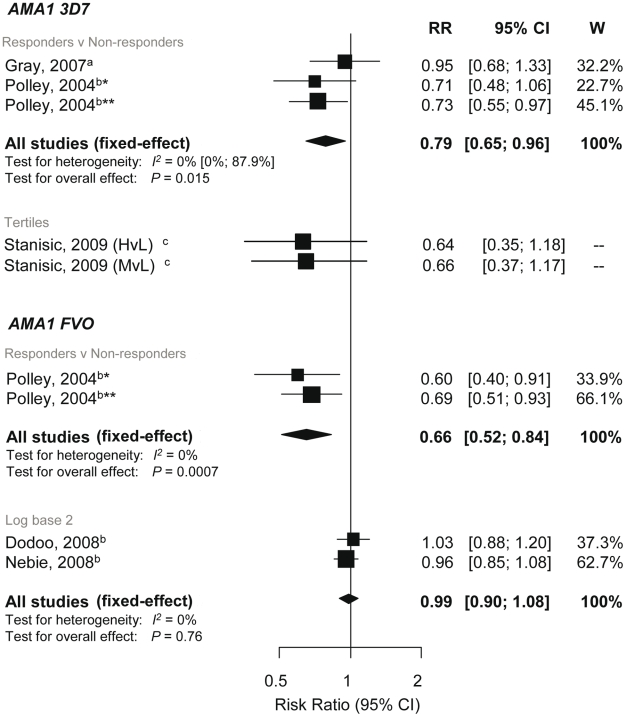
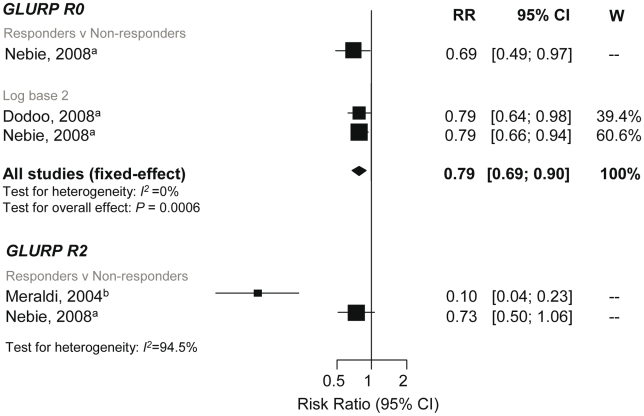
Methods and findings: We performed a systematic review with meta-analysis of prospective cohort studies examining the association between anti-merozoite immunoglobin (Ig) G responses and incidence of Plasmodium falciparum malaria. Two independent researchers searched six databases and identified 33 studies that met predefined inclusion and quality criteria, including a rigorous definition of symptomatic malaria. We found that only five studies were performed outside sub-Saharan Africa and that there was a deficiency in studies investigating antibodies to leading vaccine candidates merozoite surface protein (MSP)-1(42) and erythrocyte binding antigen (EBA)-175. Meta-analyses of most-studied antigens were conducted to obtain summary estimates of the association between antibodies and incidence of P. falciparum malaria. The largest effect was observed with IgG to MSP-3 C terminus and MSP-1(19) (responders versus nonresponders, 54%, 95% confidence interval [CI] [33%-68%] and 18% [4%-30%] relative reduction in risk, respectively) and there was evidence of a dose-response relationship. A tendency towards protective risk ratios (RR<1) was also observed for individual study estimates for apical membrane antigen (AMA)-1 and glutamate-rich protein (GLURP)-R0. Pooled estimates showed limited evidence of a protective effect for antibodies to MSP-1 N-terminal regions or MSP-1-EGF (epidermal growth factor-like modules). There was no significant evidence for the protective effect for MSP-2 (responders versus nonresponders pooled RR, MSP-2(FC27) 0.82, 95% CI 0.62-1.08, p = 0.16 and MSP-2(3D7) 0.92, 95% CI 0.75-1.13, p = 0.43). Heterogeneity, in terms of clinical and methodological diversity between studies, was an important issue in the meta-analysis of IgG responses to merozoite antigens.
Conclusions: These findings are valuable for advancing vaccine development by providing evidence supporting merozoite antigens as targets of protective immunity in humans, and to help identify antigens that confer protection from malaria. Further prospective cohort studies that include a larger number of lead antigens and populations outside Africa are greatly needed to ensure generalizability of results. The reporting of results needs to be standardized to maximize comparability of studies. We therefore propose a set of guidelines to facilitate the uniform reporting of malaria immuno-epidemiology observational studies. Please see later in the article for the Editors' Summary.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Marsh K, Kinyanjui S. Immune effector mechanisms in malaria. Parasite Immunol. 2006;28:51–60. - PubMed
-
- Cohen S, Mc GI, Carrington S. Gamma-globulin and acquired immunity to human malaria. Nature. 1961;192:733–737. - PubMed
-
- Sabchareon A, Burnouf T, Ouattara D, Attanath P, Bouharoun-Tayoun H, et al. Parasitologic and clinical human response to immunoglobulin administration in falciparum malaria. Am J Trop Med Hyg. 1991;45:297–308. - PubMed
-
- Cohen S, Butcher GA, Crandall RB. Action of malarial antibody in vitro. Nature. 1969;223:368–371. - PubMed
-
- Brown GV, Anders RF, Mitchell GF, Heywood PF. Target antigens of purified human immunoglobulins which inhibit growth of Plasmodium falciparum in vitro. Nature. 1982;297:591–593. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
