

Multiorgan detection and characterization of protease-resistant prion protein in a case of variant CJD examined in the United States
- PMID: 20098730
- PMCID: PMC2808239
- DOI: 10.1371/journal.pone.0008765
Multiorgan detection and characterization of protease-resistant prion protein in a case of variant CJD examined in the United States
Abstract
Background: Variant Creutzfeldt-Jakob disease (vCJD) is a prion disease thought to be acquired by the consumption of prion-contaminated beef products. To date, over 200 cases have been identified around the world, but mainly in the United Kingdom. Three cases have been identified in the United States; however, these subjects were likely exposed to prion infection elsewhere. Here we report on the first of these subjects.
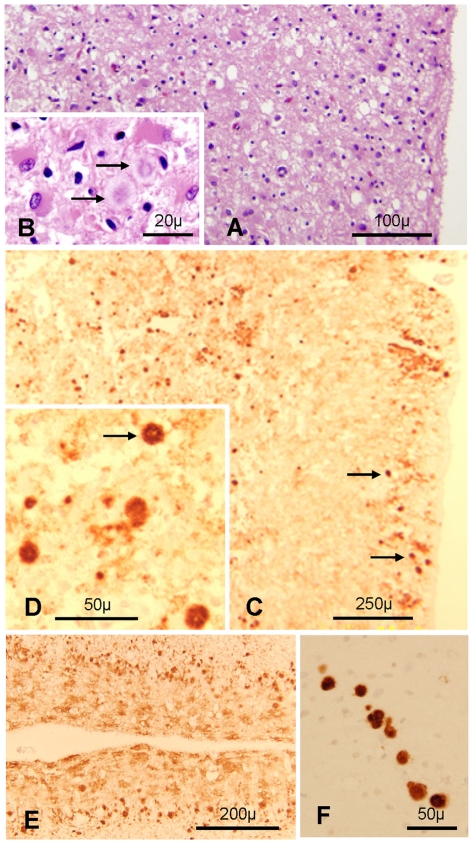
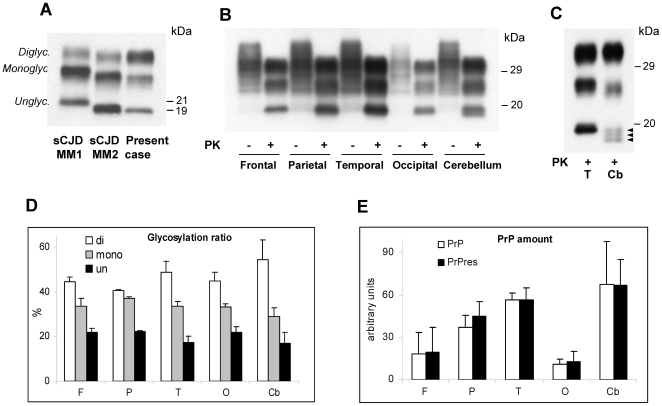
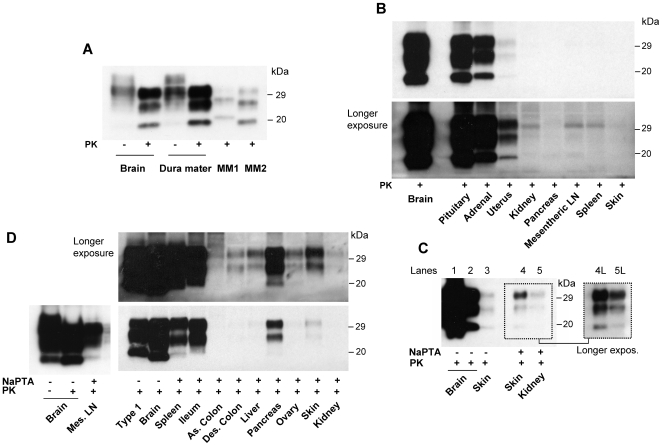
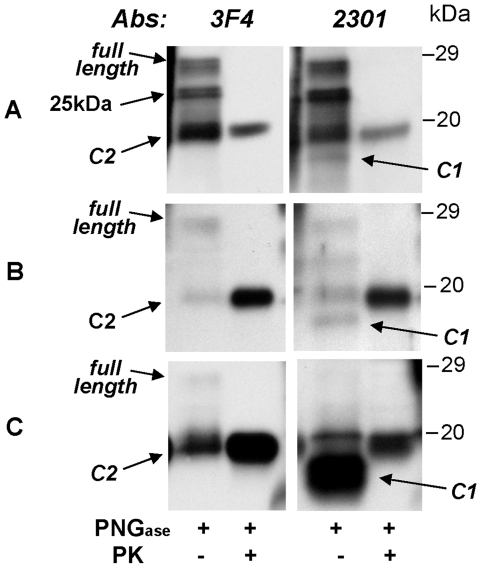
Methodology/principal findings: Neuropathological and genetic examinations were carried out using standard procedures. We assessed the presence and characteristics of protease-resistant prion protein (PrP(res)) in brain and 23 other organs and tissues using immunoblots performed directly on total homogenate or following sodium phosphotungstate precipitation to increase PrP(res) detectability. The brain showed a lack of typical spongiform degeneration and had large plaques, likely stemming from the extensive neuronal loss caused by the long duration (32 months) of the disease. The PrP(res) found in the brain had the typical characteristics of the PrP(res) present in vCJD. In addition to the brain and other organs known to be prion positive in vCJD, such as the lymphoreticular system, pituitary and adrenal glands, and gastrointestinal tract, PrP(res) was also detected for the first time in the dura mater, liver, pancreas, kidney, ovary, uterus, and skin.
Conclusions/significance: Our results indicate that the number of organs affected in vCJD is greater than previously realized and further underscore the risk of iatrogenic transmission in vCJD.
Conflict of interest statement
Figures
References
-
- Will RG, Ironside JW, Zeidler M, Cousens S, Estebeiro K, et al. A new variant of Creutzfeldt-Jakob disease in the UK. Lancet. 1996;347:921–925. - PubMed
-
- Will RG, Zeidler M, Stewart GE, Macleod MA, Ironside JW, et al. Diagnosis of new variant Creutzfeldt-Jakob disease. Ann Neurol. 2000;47:575–582. - PubMed
-
- Will RG, Ward HJ. Clinical features of variant Creutzfeldt-Jakob disease. Curr Top Microbiol Immunol. 2004;284:121–132. - PubMed
-
- Collinge J, Sidle KCL, Meads J, Ironside J, Hill AF. Molecular analysis of prion strain variation and the aetiology of ‘new variant’ CJD. Nature. 1996;383:685–690. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
