

Shaping smoking cessation in hard-to-treat smokers
- PMID: 20099951
- PMCID: PMC3623283
- DOI: 10.1037/a0018323
Shaping smoking cessation in hard-to-treat smokers
Abstract
Objective: Contingency management (CM) effectively treats addictions by providing abstinence incentives. However, CM fails for many who do not readily become abstinent and earn incentives. Shaping may improve outcomes in these hard-to-treat (HTT) individuals. Shaping sets intermediate criteria for incentive delivery between the present behavior and total abstinence. This should result in HTT individuals having improving, rather than poor, outcomes. We examined whether shaping improved outcomes in HTT smokers (never abstinent during a 10-visit baseline).
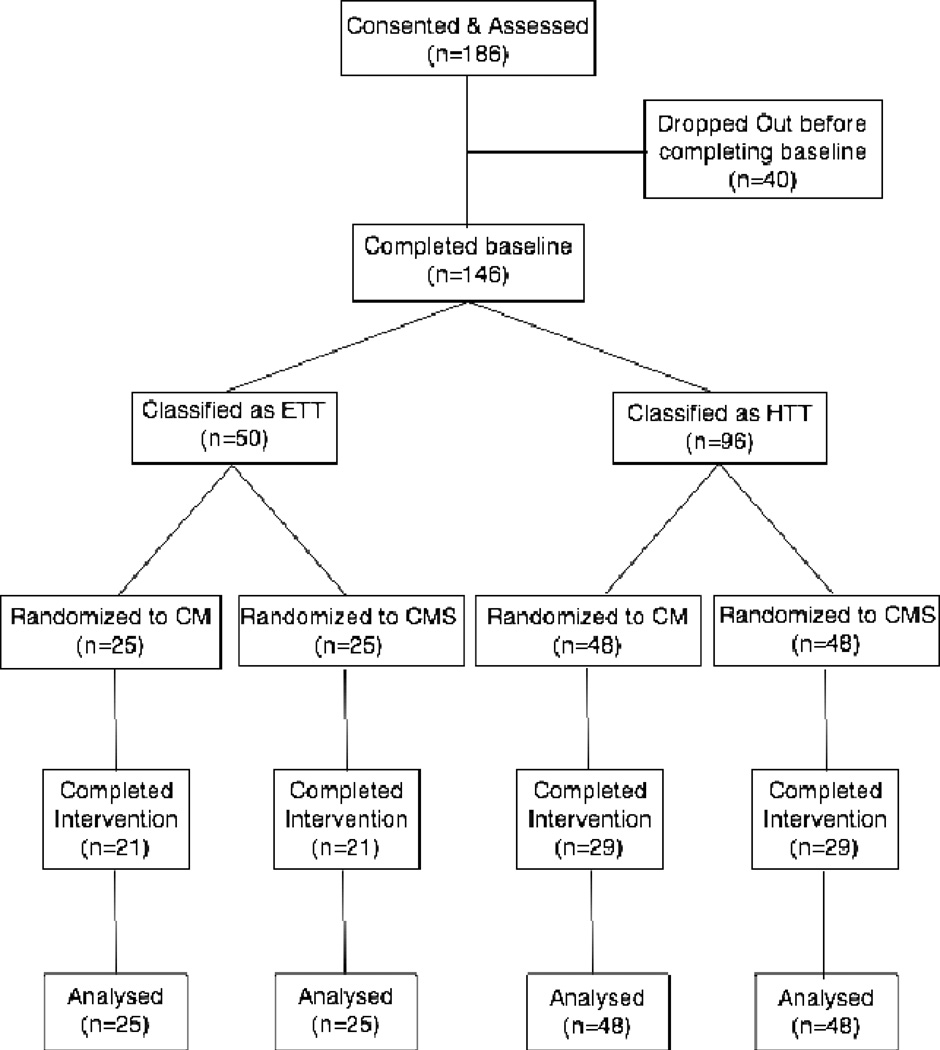
Method: Smokers were stratified into HTT (n = 96) and easier-to-treat (ETT [abstinent at least once during baseline]; n = 50) and randomly assigned to either CM or CM with shaping (CMS). CM provided incentives for breath carbon monoxide (CO) levels <4 ppm (approximately 1 day of abstinence). CMS shaped abstinence by providing incentives for COs lower than the 7th lowest of the participant's last 9 samples or <4 ppm. Interventions lasted for 60 successive weekday visits.
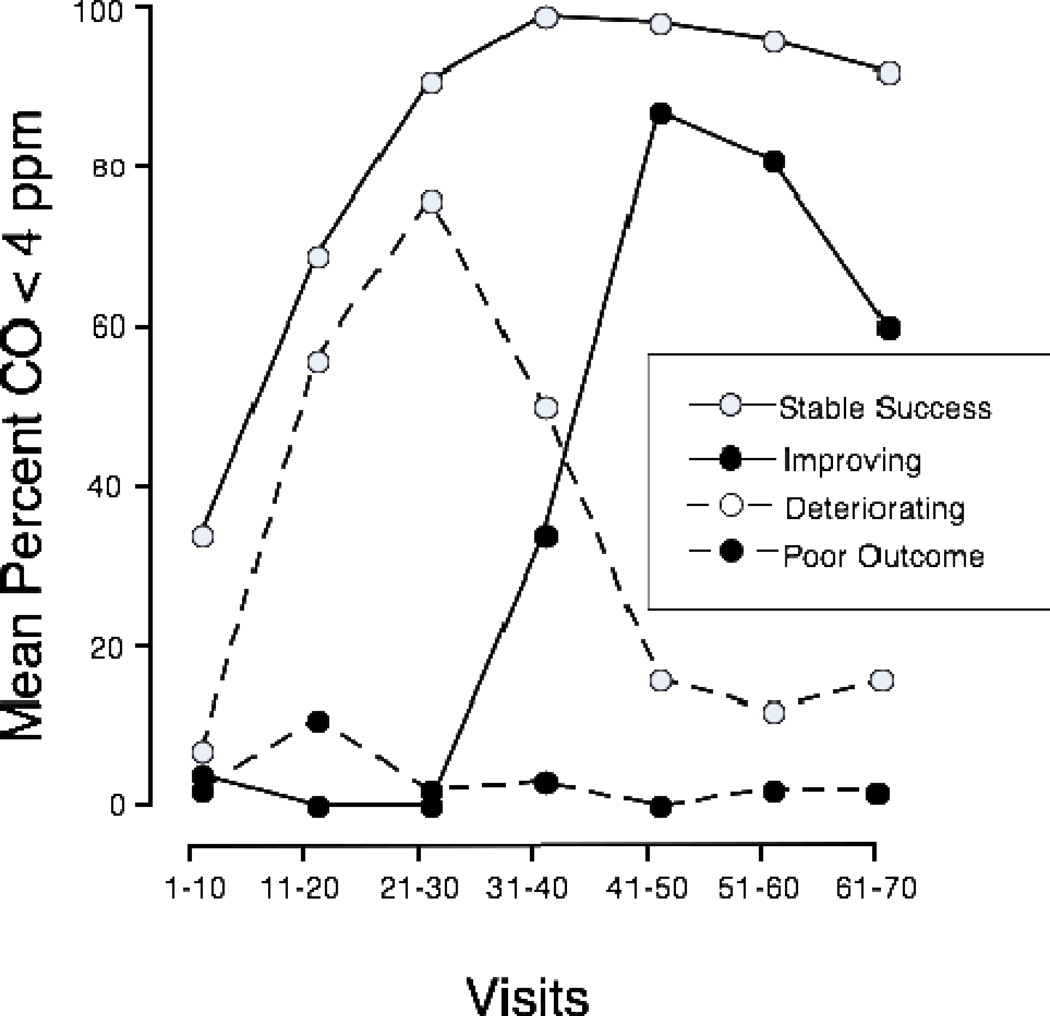
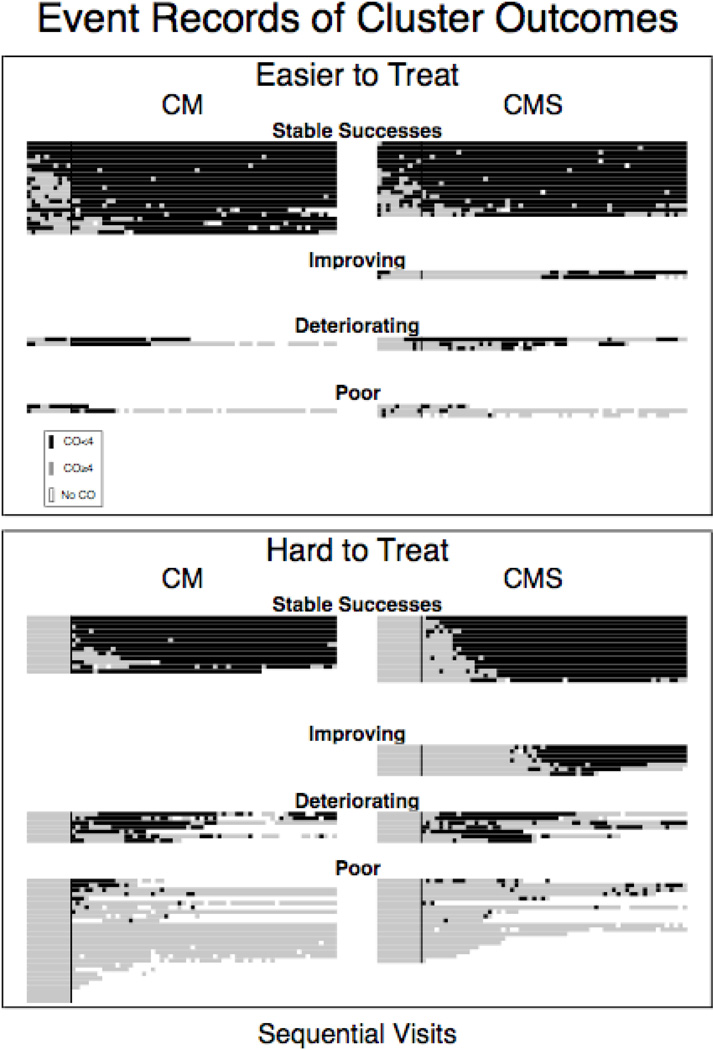
Results: Cluster analysis identified 4 groups of participants: stable successes, improving, deteriorating, and poor outcomes. In comparison with ETT, HTT participants were more likely to belong to 1 of the 2 unsuccessful clusters (odds ratio [OR] = 8.1, 95% CI [3.1, 21]). This difference was greater with CM (OR = 42, 95% CI [5.9, 307]) than with CMS, in which the difference between HTT and ETT participants was not significant. Assignment to CMS predicted membership in the improving (p = .002) as compared with the poor outcomes cluster.
Conclusion: Shaping can increase CM's effectiveness for HTT smokers.
Figures
References
-
- Amodei N, Lamb RJ. Convergent and concurrent validity of the contemplation ladder and URICA scales. Drug and Alcohol Dependence. 2004;73:301–306. - PubMed
-
- Baer JS, Lichtenstein E. Classification and prediction of smoking relapse episodes: an exploration of individual differences. Journal of Consulting & Clinical Psychology. 1988;56(1):104–10. - PubMed
-
- Biener L, Abrams DB. The Contemplation Ladder: validation of a measure of readiness to consider smoking cessation. Health Psychology. 1991;10(5):360–365. - PubMed
-
- Condiotte MM, Lichtenstein E. Self-efficacy and relapse in smoking cessation programs. Journal of Consulting and Clinical Psychology. 1981;49:648–658. - PubMed
