

Performance of 2004 American Heart Association recommendations for treatment of Kawasaki disease
- PMID: 20100771
- PMCID: PMC2896313
- DOI: 10.1542/peds.2009-0606
Performance of 2004 American Heart Association recommendations for treatment of Kawasaki disease
Abstract
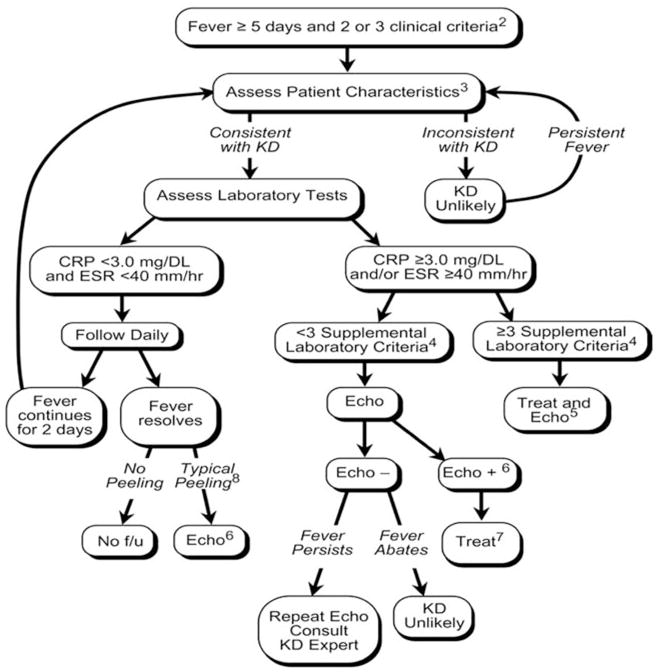
Objective: The 2004 American Heart Association (AHA) statement included a clinical case definition and an algorithm for diagnosing and treating suspected incomplete Kawasaki disease (KD). We explored the performance of these recommendations in a multicenter series of US patients with KD with coronary artery aneurysms (CAAs).
Methods: We reviewed retrospectively records of patients with KD with CAAs at 4 US centers from 1981 to 2006. CAAs were defined on the basis of z scores of >3 or Japanese Ministry of Health and Welfare criteria. Our primary outcome was the proportion of patients presenting at illness day < or =21 who would have received intravenous immunoglobulin (IVIG) treatment by following the AHA guidelines at the time of their initial presentation to the clinical center.
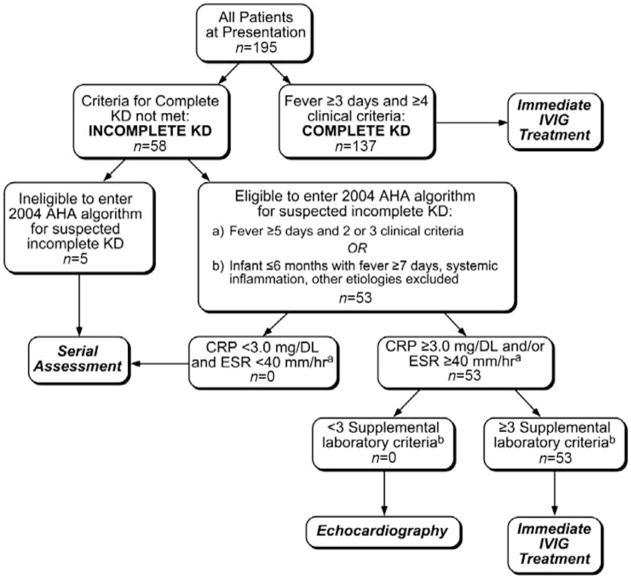
Results: Of 195 patients who met entry criteria, 137 (70%) met the case definition and would have received IVIG treatment at presentation. Fifty-three patients (27%) had suspected incomplete KD and were eligible for algorithm application; all would have received IVIG treatment at presentation. Of the remaining 5 patients, 3 were excluded from the algorithm because of fever for <5 days at presentation and 2 because of <2 clinical criteria at >6 months of age. Two of these 5 patients would have entered the algorithm and received IVIG treatment after follow-up monitoring. Overall, application of the AHA algorithm would have referred > or =190 patients (97%) for IVIG treatment.
Conclusions: Application of the 2004 AHA recommendations, compared with the classic criteria alone, improves the rate of IVIG treatment for patients with KD who develop CAAs. Future multicenter prospective studies are needed to assess the performance characteristics of the AHA algorithm in febrile children with incomplete criterion findings and to refine the algorithm further.
Figures
Similar articles
-
Kawasaki disease in Turkish children: a single center experience with emphasis on intravenous immunoglobulin resistance and giant coronary aneurysms.Turk J Pediatr. 2019;61(5):648-656. doi: 10.24953/turkjped.2019.05.002. Turk J Pediatr. 2019. PMID: 32104995
-
The Harada score in the US population of children with Kawasaki disease.Hosp Pediatr. 2014 Jul;4(4):233-8. doi: 10.1542/hpeds.2014-0008. Hosp Pediatr. 2014. PMID: 24986993
-
Efficacy and safety of intravenous immunoglobulin plus prednisolone therapy in patients with Kawasaki disease (Post RAISE): a multicentre, prospective cohort study.Lancet Child Adolesc Health. 2018 Dec;2(12):855-862. doi: 10.1016/S2352-4642(18)30293-1. Epub 2018 Oct 16. Lancet Child Adolesc Health. 2018. PMID: 30337183
-
Kawasaki disease.Rheum Dis Clin North Am. 2015;41(1):63-73, viii. doi: 10.1016/j.rdc.2014.09.010. Rheum Dis Clin North Am. 2015. PMID: 25399940 Review.
-
Kawasaki disease in adults: report of 10 cases.Medicine (Baltimore). 2010 May;89(3):149-158. doi: 10.1097/MD.0b013e3181df193c. Medicine (Baltimore). 2010. PMID: 20453601 Review.
Cited by
-
Kawasaki Disease: A Clinician's Update.Int J Pediatr. 2013;2013:645391. doi: 10.1155/2013/645391. Epub 2013 Oct 27. Int J Pediatr. 2013. PMID: 24282419 Free PMC article. Review.
-
Diagnostic characteristics of supplemental laboratory criteria for incomplete Kawasaki disease in children with complete Kawasaki disease.Korean J Pediatr. 2015 Oct;58(10):369-73. doi: 10.3345/kjp.2015.58.10.369. Epub 2015 Oct 21. Korean J Pediatr. 2015. PMID: 26576180 Free PMC article.
-
Increased incidence of incomplete Kawasaki disease at a pediatric hospital after publication of the 2004 American Heart Association guidelines.Pediatr Cardiol. 2012 Oct;33(7):1097-103. doi: 10.1007/s00246-012-0232-9. Epub 2012 Feb 15. Pediatr Cardiol. 2012. PMID: 22349679
-
The time option of IVIG treatment is associated with therapeutic responsiveness and coronary artery abnormalities but not with clinical classification in the acute episode of Kawasaki disease.Pediatr Rheumatol Online J. 2019 Jul 31;17(1):53. doi: 10.1186/s12969-019-0352-3. Pediatr Rheumatol Online J. 2019. PMID: 31366406 Free PMC article.
-
Incomplete and atypical Kawasaki disease: a clinicopathologic paradox at high risk of sudden and unexpected infant death.Pediatr Cardiol. 2012 Jun;33(5):802-5. doi: 10.1007/s00246-012-0186-y. Epub 2012 Feb 10. Pediatr Cardiol. 2012. PMID: 22322565
References
-
- Kato H, Sugimura T, Akagi T, et al. Long-term consequences of Kawasaki disease: a 10- to 21-year follow-up study of 594 patients. Circulation. 1996;94(6):1379–1385. - PubMed
-
- Furusho K, Kamiya T, Nakano H, et al. High-dose intravenous gammaglobulin for Kawasaki disease. Lancet. 1984;2(8411):1055–1058. - PubMed
-
- Newburger JW, Takahashi M, Burns JC, et al. The treatment of Kawasaki syndrome with intravenous gamma globulin. N Engl J Med. 1986;315(6):341–347. - PubMed
-
- Sonobe T, Kiyosawa N, Tsuchiya K, et al. Prevalence of coronary artery abnormality in incomplete Kawasaki disease. Pediatr Int. 2007;49(4):421–426. - PubMed
-
- Newburger JW, Takahashi M, Gerber MA, et al. Diagnosis, treatment, and long-term management of Kawasaki disease: a statement for health professionals from the Committee on Rheumatic Fever, Endocarditis and Kawasaki Disease, Council on Cardiovascular Disease in the Young, American Heart Association. Circulation. 2004;110(17):2747–2771. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
