

Myocardial infarction and stroke associated with diuretic based two drug antihypertensive regimens: population based case-control study
- PMID: 20100777
- PMCID: PMC2811239
- DOI: 10.1136/bmj.c103
Myocardial infarction and stroke associated with diuretic based two drug antihypertensive regimens: population based case-control study
Abstract
Objective: To examine the association of myocardial infarction and stroke incidence with several commonly used two drug antihypertensive treatment regimens. Design Population based case-control study. Setting Group Health Cooperative, Seattle, WA, USA.
Participants: Cases (n=353) were aged 30-79 years, had pharmacologically treated hypertension, and were diagnosed with a first fatal or non-fatal myocardial infarction or stroke between 1989 and 2005. Controls (n=952) were a random sample of Group Health members who had pharmacologically treated hypertension. We excluded individuals with heart failure, evidence of coronary heart disease, diabetes, or chronic kidney disease. Exposures One of three common two drug combinations: diuretics plus beta blockers; diuretics plus calcium channel blockers; and diuretics plus angiotensin converting enzyme inhibitors or angiotensin receptor blockers.
Main outcome measures: Myocardial infarction or stroke.
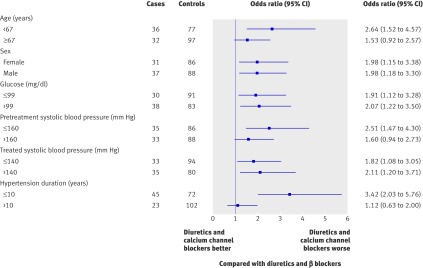
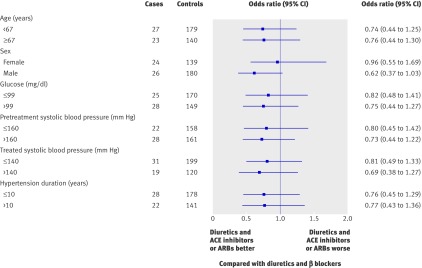
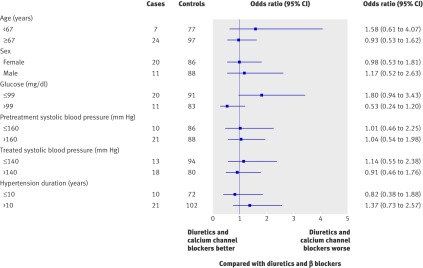
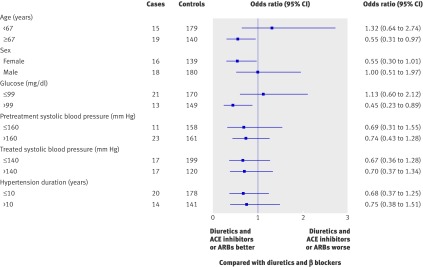
Results: Compared with users of diuretics plus beta blockers, users of diuretics plus calcium channel blockers had an increased risk of myocardial infarction (adjusted odds ratio (OR) 1.98, 95% confidence interval 1.37 to 2.87) but not of stroke (OR 1.02, 95% CI 0.63 to 1.64). The risks of myocardial infarction and stroke in users of diuretics plus angiotensin converting enzyme inhibitors or angiotensin receptor blockers were slightly but not significantly lower than in users of diuretics plus beta blockers (myocardial infarction: OR 0.76, 95% CI 0.52 to 1.11; stroke: OR 0.71, 95% CI 0.46 to 1.10).
Conclusions: In patients with hypertension, diuretics plus calcium channel blockers were associated with a higher risk of myocardial infarction than other common two drug treatment regimens. A large trial of second line antihypertensive treatments in patients already on low dose diuretics is required to provide a solid basis for treatment recommendations.
Conflict of interest statement
Competing interests: All authors have completed the Unified Competing Interest form at
Figures
Comment in
-
Antihypertensive regimens. Should beta blockers be second line treatment?BMJ. 2010 Feb 23;340:c1065. doi: 10.1136/bmj.c1065. BMJ. 2010. PMID: 20179113 No abstract available.
-
The use of diuretics plus calcium channel blockers for hypertension may be associated with a higher risk of myocardial infarction but not stroke compared with the combination of diuretics plus beta blockers.Evid Based Med. 2010 Jun;15(3):92-3. doi: 10.1136/ebm1067. Evid Based Med. 2010. PMID: 20522694 Free PMC article. No abstract available.
References
-
- ALLHAT officers and coordinators for the ALLHAT Collaborative Research Group. Major outcomes in high-risk hypertensive patients randomized to angiotensin-converting enzyme inhibitor or calcium channel blocker vs diuretic: the antihypertensive and lipid-lowering treatment to prevent heart attack trial (ALLHAT). JAMA 2002;288:2981-97. - PubMed
-
- Psaty BM, Lumley T, Furberg CD, Schellenbaum G, Pahor M, Alderman MH, et al. Health outcomes associated with various antihypertensive therapies used as first-line agents: a network meta-analysis. JAMA 2003;289:2534-44. - PubMed
-
- Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL Jr, et al for the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. National Heart, Lung, and Blood Institute, National High Blood Pressure Education Program Coordinating Committee. Seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure. Hypertension 2003;42:1206-52. - PubMed
-
- National Collaborating Centre for Chronic Conditions. Hypertension: management in adults in primary care—pharmacological update. Royal College of Physicians, 2006. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases